
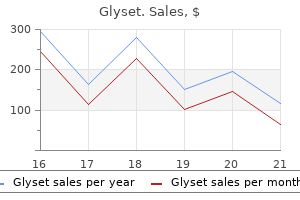
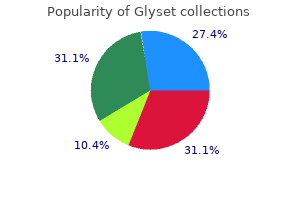
Glyset
Mike Larvin BSc MBBS FRCS MD
- Professor of surgery, Consultant upper GI
- and pancreatic surgeon and Head of division
- Academic Division of Surgery, School of
- Graduate Entry Medicine and Health, Derby
- City General Hospital, Derby, UK
Glyset dosages: 50 mg
Glyset packs: 30 pills, 60 pills, 90 pills

Buy glyset 50mg online
In the past cheap glyset 50mg visa, anemia was handled with pink blood cell transfusions order glyset 50 mg, a treatment that would trigger iron overload or sensitization to future transplants and which conferred dangers of infections similar to hepatitis B and C cheap glyset 50 mg online. Since there have been no direct comparisons of the two treatment lessons, treatment of anemia varies significantly relying on patient traits and provider preferences. Clinical practice tips for anemia in continual kidney illness: problems and options. Advantages embrace longer affected person survival, less morbidity, cost savings, and improved high quality of life compared with dialysis. Living kidney donation stays the most effective remedy, with average graft survival of roughly 12 to 15 years, with longer survival for well-matched sibling transplants. This good news is tempered by the reality that demand for transplant kidneys far exceeds the supply of accessible organs. Recipient Evaluation the objectives of evaluating a potential recipient should be to determine potential barriers to transplantation, determine treatable circumstances that might attenuate the danger of the surgery or immunosuppression, and explain the advantages and dangers. Comorbid situations and the results of immunosuppression on these conditions are thought-about. Patient age older than 50 years, 263 264 Chapter 13 the Patient with a Kidney Transplant diabetes, abnormal electrocardiogram, angina, or congestive heart failure have been demonstrated as predictors of cardiac demise and nonfatal cardiac occasions with kidney transplantation. Noninvasive strategies corresponding to thallium perfusion imaging and dobutamine stress echo have demonstrated the ability to predict cardiac events and will prevent high-risk sufferers from requiring angiography. In patients with malignancies, a 2- to 5-year remission could additionally be required before transplantation depending on tumor sort, invasiveness, and prior treatment. Although obesity is a danger for wound-related problems, long-term outcomes are much like nonobese sufferers until cardiovascular disease exists. Imaging or functional evaluation of the kidneys and lower urinary tract may be essential in certain sufferers. After a affected person has been accepted as a candidate, she or he is added to the transplant waiting record, at which period initial medical screening of potential residing kidney donors can take place. A affected person on the waiting record for greater than 1 12 months should be seen periodically to replace his or her situation. Although the dangers of kidney donation are small, these dangers have to be rigorously explained to a potential dwelling donor. Infection, bleeding, and different postoperative problems happen in up to 15% of patients. Mild blood stress elevation and proteinuria after donation has been reported in some research but not all, and the long-term penalties are at present unclear. Donors are rigorously screened for kidney disease to forestall the potential of loss of operate in the remaining kidney. Hypertension, proteinuria, obesity, kidney stones, and structural Chapter thirteen the Patient with a Kidney Transplant 265 or practical kidney illness are all relative contraindications to donation depending on severity. When recipients are affected by hereditary issues such as polycystic kidney disease or hereditary nephritis, the condition should be dominated out in related donors either clinically or with genetic testing. Donors with hepatitis C are generally accepted for hepatitis C�positive recipients. A combination of factors corresponding to hypertension, superior age, elevated serum creatinine, oliguria, or dependence on pressor assist may exclude a donor. They are generally utilized in recipients with traits associated with poor dialysis survival such as superior age or diabetes. Predictors of Outcome Recipient elements, donor elements, and donor/recipient compatibility all influence long-term graft survival. Race and ethnicity could affect graft survival for both donors and recipients, with nonblack donor kidneys and nonblack, non-Hispanic recipients of grafts having the longest graft survival. Kidneys from residing associated or unrelated donors survive longer on average than deceased donor kidneys, as do kidneys from youthful compared with older donors. Immunology A primary evaluate of the mechanisms of immune recognition and response to an allograft is useful to better understand the affected person who has undergone kidney transplantation as nicely as the pharmacologic brokers used to prevent allograft rejection. Although advances in immunosuppression have narrowed advantages for well-matched transplants, a two-haplotype equivalent transplant from a family member or a zero-antigen mismatched deceased donor transplant confers a graft survival profit in contrast with transplants with lesser degrees of matching. T cells T cells are processed in the thymus and are central to mobile immunity and allograft recognition and rejection. These properties make them a typical target of medicine designed to forestall rejection. They then initiate an immune response to international peptides by secreting cytokines necessary in B-cell proliferation and activation and cytotoxic T-cell activation. Although sign 1 alone will trigger anergy, the addition of signal 2, also called costimulation, will result in an immune response. B Cells B cells develop at multiple sites of the body, together with the liver, spleen, and lymph nodes. Antibody-mediated mobile cytotoxicity happens through complement fixation and subsequent cell lysis. Pharmacotherapy In the Nineteen Sixties and 1970s the first transplant immunosuppressive brokers consisted of steroids and azathioprine. Since that time the variety of obtainable 268 Chapter thirteen the Patient with a Kidney Transplant immunosuppressive agents has elevated tremendously. Agents can be utilized for desensitization therapy prior to transplant, induction remedy on the time of transplant, maintenance remedy to prevent rejection of the allograft, or the remedy of acute rejection. There is a large diploma of overlap between indications, and lots of brokers are used "off-label. These preparations neutralize lymphocytes by a number of antibody-mediated mechanisms, with a sustained impact on proliferation, and are simpler than basiliximab in preventing acute rejection. Toxicities are associated to immunosuppression, heterogeneity of preparations, allergic or anaphylactoid responses to nonhuman preparations, and cytopenias. Furthermore, a change in sort and timing of rejection could additionally be seen, including monocyte-induced and humoral rejections occurring past the early posttransplant months. Dosing is adjusted according to trough or peak blood levels and varies depending on immunosuppressive routine (see Section V. Chapter thirteen the Patient with a Kidney Transplant 271 hypertriglyceridemia, hypercholesterolemia, cytopenias, pneumonitis, delayed wound healing, lymphoceles, diarrhea, and proteinuria, in addition to potentiation of calcineurin inhibitor toxicity. As with calcineurin inhibitors, dosing is adjusted in accordance with trough or peak blood levels and varies relying on immunosuppressive regimen (see Section V. Azathioprine offers less selective lymphocyte inhibition and could be associated with cytopenias and neoplasias. Corticosteroids are used throughout induction, as maintenance therapy, and for the therapy of acute rejection. Their effectiveness is difficult by a wide range of well-known unwanted effects, including hypertension, glucose intolerance, weight achieve, cataracts, poor wound healing, osteoporosis, and osteonecrosis. Although corticosteroid withdrawal and avoidance have been explored (see Section V. Corticosteroids and antithymoctye globulin (described within the earlier sections) are used in cell-mediated (T-cell) rejection.
Order glyset 50mg on-line
Family: Togaviridae the classification of viruses has undergone nice change buy glyset 50 mg without prescription, as has bacterial taxonomy discount glyset 50mg amex. Estimates recommend that more than 30 purchase 50mg glyset free shipping,000 viruses are being studied in laboratories and reference centers worldwide. The classification and viral info presented right here fol lows the outline given in Chapter 10 Tables 10. In formation additionally could be present in Human Virology: A Text for Students of Medicine, Dentistry, and Microbiology (L. The 21 families of viruses listed below are primarily people who infect vertebrates. Thus, these families represent solely a small part of the 108 families and unassigned genera and more than 5,000 viruses recognized in Virus Taxonomy-Seventh Report of the International Committee on Taxonomy of Viruses, van Regenmortal et al. Synthesis oc curs in the host cell cytoplasm; maturation includes budding of nucleocapsids by way of the host cell plasma membrane. Family: Caliciviridae Genera: Flavivirus (yellowfever virus, dengue fever virus, St. Synthesis oc curs within the host cell cytoplasm; maturation entails budding by way of host cell endoplasmic reticulum and Golgi equipment membranes. Synthesis happens within the host cell cytoplasm; maturation includes budding via membranes of the endoplasmic reticulum and Golgi equipment. Synthesis happens in the host cell nucleus; maturation occurs through budding from the host cell plasma membrane. Syn thesis occurs within the host cell nucleus; maturation takes place in the host cell cytoplasm. Synthesis occurs in the host cell cytoplasm; maturation involves budding from the host cell plasma membrane. These viruses are 'Biosafety Level 4' pathogens-they have to be handled in the laboratory beneath max imum containment conditions. Synthesis happens in the host cell cytoplasm; maturation occurs within the Golgi equipment. Synthesis occurs within the host cell cytoplasm; maturation involves budding through the host cell plasma membrane. Syn thesis occurs in the host cell cytoplasm; maturation involves budding from the host cell plasma membrane. The human pathogens Lassa, Machupo, and Junin viruses are 'Biosafety Level four' pathogens-they should be han dled in the laboratory under most containment situations. Family: Hepadnaviridae Genera: Orthoreovirus (reoviruses 1, 2, and 3) Orbivirus (Orungo virus) Rotavirus (human rotaviruses) Cypovirus (cytoplasmic polyhidrosis viruses) Coltivirus (Colorado tick fever virus) Plant reovirus 1/3 (plant reoviruses subgroups 1, 2, and 3) Each genus differs in morphology and physiochemical details. Syn thesis and maturation happen in quickly dividing host cells, specifi cally within the host cell nucleus. Synthesis and maturation oc cur within the host cell nucleus, with budding via the nuclear envelope. Although most herpesviruses trigger persistent infec tions, virions may be released by rupture of the host cell plasma membrane. Syn thesis and maturation take place within the portion of the host cell cytoplasm called viroplasm ('viral factories'). Immediately and thoroughly wash hands and other pores and skin sur faces which may be contaminated with blood, physique fluids comprise ing seen blood, or other body fluids to which universal pre cautions apply. Some institutions have relaxed recommendations for us ing gloves for phlebotomy procedures by skilled phlebotomists in settings the place the prevalence of bloodborne pathogens is known to be very low (for example, volunteer blooddonation centers). Gloves should at all times be obtainable to well being care workers who wish to use them for phlebotomy. In addition, the next basic guidelines apply: Concern for maintaining safe situations at school and hospital laboratories, in different work settings, and especially during pa tient interactions has led the federal authorities to formulate numerous regulations and proposals. These are far too ex tensive to reproduce right here in their entirety; a quantity of are almost 200 pages lengthy. As an introduction to the kinds of safety mea sures that should be taken, a number of of the rules set forth in these publications are provided beneath. These blood and body fluid precautions as they pertain to all patients are referred to as 'Universal Blood and Body Fluid Precautions,' or extra simply as 'Universal Precautions. Use gloves for performing phlebotomy when the well being care worker has cuts, scratches, or different breaks in his/her skin. Use gloves in situations the place the health care employee judges that hand contamination with blood could occur, for instance, when performing phlebotomy on an uncooperative affected person. Both publications present very detailed information about proce dures that should be followed. Take care to prevent injuries when using needles, scalpels, and other sharp instruments or gadgets; when dealing with sharp in struments after procedures; when cleaning used instruments; and when disposing of used needles. Place used disposable syringes and needles, scalpel blades, and other sharp objects in puncture resistant containers for disposal. Use protective limitations to prevent publicity to blood, body fluids containing visible blood, and other fluids to which uni versal precautions apply. The type of protective barrier(s) must be appropriate for the process being performed and the kind of publicity anticipated. Steps eight & 9: the remaining phosphate group is moved from the end to the middle carbon atom by phosphoglycerate mutase, and a molecule of water is removed by enolase. Each of the 10 steps of glycolysis is catalyzed by a specific enzyme, which is indicated in a purple oval. It supplies an alternate pathway for the breakdown of glucose as properly as pentoses (five-carbon sugars). This pathway performs three necessary roles: (1) It supplies intermediate pentoses, particularly ribose, that the bacterial cell should use to synthesize nucleic acids. For clarity, the particular enzymes catalyzing these reactions and the structural formulation of substrates have been omitted. Pyruvic acid (from glycolysis) Stage F the final stage of the Krebs cycle entails three steps to regenerate oxaloacetic acid by the oxidation of succinic acid. The -ketoglutarate dehydrogenase complex consists of three enzymes and works very like the pyruvate dehydrogenase complicated that varieties acetyl-CoA. This reaction is catalyzed by a pyruvate dehydrogenase complex, which accommodates three enzymes. Each of the eight steps of the Krebs cycle is also catalyzed by a particular enzyme, as indicated in a purple oval. The other 10 three-carbon molecules are recycled (steps 4 through 6), forming 6 five-carbon molecules. The enzyme catalyzing this step is ribulose diphosphate carboxylase, probably the most prevalent enzyme within the organic world. Two filo-viruses, the Ebola virus and the Marburg virus, have been related to human illness filter paper technique Method of evaluating the antimicrobial properties of a chemical agent utilizing filter paper disks placed on an inoculated agar plate filtration (1) A methodology of estimating the size of bacterial populations by which a known quantity of air or water is drawn through a filter with pores too small to allow passage of bacteria.
Diseases
- Dextrocardia-bronchiectasis-sinusitis
- Peripheral neuropathy
- Factor XIII deficiency
- X-linked agammaglobulinemia
- Xerocytosis, hereditary
- Arc syndrome
- Free sialic acid storage disease
Buy 50 mg glyset mastercard
Erythema multiforme: a evaluation of its characteristics purchase glyset 50 mg online, diagnostic standards discount 50 mg glyset overnight delivery, and administration purchase 50mg glyset with visa. Stevens�Johnson syndrome and poisonous epidermal necrolysis are severity variants of the identical disease which differs from erythema multiforme. Erythema multiforme in children: uncommon clinical options with seasonal incidence. Controversy: are systemic steroids indicated within the remedy of erythema multiforme A doubleblind, placebo-controlled trial of steady acyclovir therapy in recurrent erythema multiforme. Management of childhood urticaria: present data and sensible recommendations. Safety of cetirizine in infants 6 to 11 months of age: a randomized, double-blind, placebo-controlled research. Safety and tolerability of levocetirizine dihydrochloride in infants and kids with allergic rhinitis or chronic urticaria. Hereditary angioedema: new findings regarding symptoms, affected organs, and course. Autoinflammatory syndromes and mobile responses to stress: pathophysiology, diagnosis and new therapy perspectives. The spectrum of acquired and familial cold-induced urticaria/ urticaria-like syndromes. Muckle� Wells syndrome: scientific and histological skin findings compatible with cold air urticaria in a big kindred. Neonatalonset multisystem inflammatory disorder: the emerging function of pyrin genes in autoinflammatory ailments. The expanding spectrum of systemic autoinflammatory issues and their rheumatic manifestations. A just lately recognised persistent inflammatory illness of early onset characterised by the triad of rash, central nervous system involvement and arthropathy. The spectrum of monogenic autoinflammatory syndromes: understanding illness mechanisms and use of focused therapies. Chronic infantile neurological cutaneous articular syndrome in a patient from Japan. Interleukin-1 blockade by anakinra improves medical signs in sufferers with neonatalonset multisystem inflammatory illness. An autoinflammatory illness with deficiency of the interleukin-1-receptor antagonist. Mutations in proteasome subunit sort 8 trigger chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperature with evidence of genetic and phenotypic heterogeneity. Eosinophilic fasciitis and eosinophilic cellulitis in a affected person with irregular circulating clonal T cells: increased production of interleukin 5 and inhibition by interferon alfa. Eosinophilic cellulitis as a cutaneous manifestation of idiopathic hypereosinophilic syndrome. Eosinophilic annular erythema: an expression of the medical and pathological polymorphism of Wells syndrome. Eosinophilic annular erythema is a peculiar subtype in the spectrum of Wells syndrome: a multicentre long-term follow-up research. Sweet syndrome because the presenting manifestation of continual granulomatous illness in an toddler. Pediatric Sweet syndrome and immunodeficiency efficiently handled with intravenous immunoglobulin. Myocarditis and coronary dilatation within the 1st week of life: neonatal incomplete Kawasaki disease Diagnosis, therapy, and long-term administration of Kawasaki illness: a statement for well being professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Maculopapular rash in the convalescent section of Kawasaki illness: case sequence and literature evaluation. Development of psoriatic lesions throughout acute and convalescent phases of Kawasaki disease. Annular pustules in Kawasaki illness: a further case indicating the affiliation with psoriasis Clinical options of patients with Kawasaki illness whose mother and father had the same disease. Discrimination between incomplete and atypical Kawasaki syndrome versus different febrile diseases in childhood: results from a world registry-based examine. Diagnosis, remedy and outcome of Kawasaki illness in an Australian tertiary setting: a evaluation of three years expertise. National survey of coronary artery bypass grafting for coronary stenosis brought on by Kawasaki illness in Japan. Mortality amongst persons with a history of Kawasaki illness in Japan: can paediatricians safely discontinue follow-up of children with a historical past of the illness however without cardiac sequelae Mortality amongst persons with a history of Kawasaki disease in Japan: the fifth look. Report from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease within the Young, American Heart Association. Mortality amongst individuals with a history of Kawasaki disease in Japan: existence of cardiac sequelae elevated the mortality. Prevalence of coronary artery abnormalities in Kawasaki illness is extremely depending on gamma globulin dose but unbiased of salicylate dose. The prevention of coronary artery aneurysm in Kawasaki disease: a meta- analysis on the efficacy of aspirin and immunoglobulin remedy. Evaluation of the efficacy of treatment of Kawasaki disease before day 5 of illness. Early intravenous gamma-globulin remedy for Kawasaki illness: the nationwide surveys in Japan. Late intravenous gamma globulin therapy in infants and youngsters with Kawasaki disease and coronary artery abnormalities. Kawasaki disease: an evidence based mostly approach to prognosis, treatment, and proposals for future research. Corticosteroids within the initial treatment of Kawasaki illness: Report of a randomized trial. Effect of corticosteroids along with intravenous gamma globulin therapy on serum cytokine levels within the acute part of Kawasaki illness in kids. Intravenous immunoglobulin plus corticosteroid to forestall coronary artery abnormalities in Kawasaki illness: a meta-analysis. Steroid pulse remedy for children with intravenous immunoglobulin therapy-resistant Kawasaki disease: a prospective examine.
Buy glyset 50mg
Laboratory investigation might reveal an elevated erythrocyte sedimentation price buy glyset 50mg with visa, eosinophilia buy 50mg glyset fast delivery, and hypocomplementemia (C3 is lowered whereas C4 stays normal) generic 50 mg glyset visa. Thrombotic microangiopathies are characterized by a microangiopathic hemolytic anemia, thrombocytopenia, and variable renal and neurologic manifestations. These problems start with endothelial damage followed by secondary platelet thrombi formation in renal arterioles; renal cortical necrosis might result from the arterial lesions. The primary website of harm is the glomerulus or the vascular supply of the glomerulus; the proximal tubule and interstitium are relatively uninvolved. Malignant hypertension inflicting a thrombotic microangiopathy is characterized by hypertension related to papilledema and/or retinal hemorrhages; different organ involvement might manifest as chest ache, shortness of breath from pulmonary edema, and confusion from brain involvement. Scleroderma renal disaster should be considered in patients with scleroderma and an abrupt rise in serum creatinine related to hypertension. Nephrotic glomerular issues are characterized by a urine protein excretion of higher than three g in 24 hours. Clinical signs and signs characteristic of a nephrotic dysfunction embrace pitting peripheral edema, hypertension, periorbital edema, and anasarca. Nephritic glomerular issues are characterised by hematuria and proteinuria (typically 1 to 2 g in 24 hours). Clinical symptoms and signs that recommend that the glomerulonephritis is part of a systemic disease include palpable purpura, skin rash, arthralgias, arthritis, fever, cardiac murmurs, sinusitis, hemoptysis, belly ache, and acute neuropathy. Hypocomplementemia is frequent in postinfectious glomerulonephritis, lupus nephritis, membranoproliferative glomerulonephritis, and combined cryoglobulinemia. It is important to acknowledge that different nonrenal situations may decrease serum complement levels. Physical findings with acute drug-induced interstitial nephritis may be missing, although fever and a maculopapular or petechial skin eruption may happen with any of the brokers, notably the penicillin derivatives and allopurinol. However, this discovering could additionally be missing, and different scientific clues might be essential to make the analysis. To distinguish between the 2, numerous diagnostic indices and formulae have been developed primarily based on their pathophysiologic differences. The increased reabsorption of water will increase urine particular gravity and osmolality. The incidence of nephrotoxicity correlates higher with whole cumulative dose than with plasma ranges. Predisposing elements are old age, preexisting renal disease, volume depletion, and mixture with other brokers. Nephrotoxicity is normally clinically obvious after 5 to 10 days of remedy; early findings are isosthenuria brought on by nephrogenic diabetes insipidus, and magnesium and potassium losing. It is recommended that, in sufferers with regular kidney operate in regular state, aminoglycosides are administered as a single dose day by day somewhat than multiple-dose daily therapy regimens. It can additionally be instructed that aminoglycoside drug ranges are monitored when therapy with single every day dosing is used for greater than 48 hours. Serum creatinine typically peaks at 3 to four days and returns to baseline after a few week. Chapter 10 the Patient with Acute Kidney Injury 227 Although numerous brokers have been studied to stop distinction nephropathy, the only therapies which were shown to be beneficial are intravenous hydration with both isotonic saline or isotonic sodium bicarbonate before and after the contrast load. Rhabdomyolysis is brought on by muscle injury (traumatic or atraumatic) that leads to the systemic release of muscle contents including myoglobin. Rhabdomyolysis must be thought-about in sufferers with trauma, muscle pain, and dark brown urine. Laboratory clues to the analysis include a rapid rise of serum creatinine, massively increased creatine phosphokinase, hyperphosphatemia, hyperuricemia, hypocalcemia, elevated anion gap, and disproportionate hyperkalemia. Serum calcium is lowered as a outcome of the sequestration of calcium into injured muscle; this calcium is launched from the tissue in the course of the restoration phase and will trigger hypercalcemia. Therefore, replacement of serum calcium must be prevented until signs of hypocalcemia are present. The solely proven therapy in the remedy of rhabdomyolysis is early and vigorous infusion of intravenous isotonic saline. Mannitol administration and urinary alkalinization are sometimes attempted in the treatment of rhabdomyolysis, although their efficacy will not be superior to vigorous hydration with saline alone. Theoretically, forced diuresis with mannitol may aid in the washout of obstructing myoglobin pigment. Mannitol administration could additionally be attempted only after the correction of quantity deficits; saline and mannitol ought to be administered along with a objective urine output of 300 mL/hour. Urinary alkalinization may inhibit myoglobin precipitation; however, urinary alkalinization is troublesome to achieve in follow and requires the administration of a big quantity of bicarbonate. Bicarbonate administration in rhabdomyolysis carries the danger of worsening hypocalcemia due to increased calcium and phosphorus precipitation into injured muscle. Thus, mannitol and urinary alkalinization ought to be utilized cautiously, if at all, within the management of rhabdomyolysis. The condition sometimes happens during induction chemotherapy for malignancies with excessive cell turnover. Clinical features of acute uric acid nephropathy are hyperuricemia, hyperkalemia, hyperphosphatemia, and a urine urate to creatinine ratio larger than 1. Preventive measures include allopurinol administration (300 to 600 mg/day) and vigorous hydration and forced diuresis with mannitol. Alkalinization of the urine has been traditionally really helpful, but has not been proved more useful than saline administration alone; additionally, bicarbonate therapy carries the danger of elevated calcium precipitation. Rasburicase, a recombinant urate oxidase, can lower uric acid ranges quickly allowing earlier Chapter 10 the Patient with Acute Kidney Injury 229 institution of chemotherapy, and may cut back the danger of acute uric acid nephropathy. Oral or enema sodium phosphosoda therefore is contraindicated in patients with kidney illness. Shape/Appearance Needle formed Envelope formed Diamond shaped, yellow or brown Needle shaped or shocks of wheat Needle formed, birefringent Needle formed, often forming rosettes Uric acid Sulfadiazine Acyclovir Indinavir sulfate or atazanavir 230 Chapter 10 the Patient with Acute Kidney Injury Table 10-11. All supportive measures, together with dialysis, must be used as warranted by the medical scenario. Glomerulonephritis and liver cirrhosis are associated with cryoglobulinemia, IgA nephropathy, membranous glomerulonephritis (associated with hepatitis B), and membranoproliferative glomerulonephritis (associated with hepatitis C). A renal biopsy in such circumstances could provide the 232 Chapter 10 the Patient with Acute Kidney Injury basis and justification for aggressive and life-saving remedy. When 1 L of isotonic crystalloid is given, roughly 250 mL stays in the plasma compartment, whereas 750 mL enters the interstitial compartment. After a bolus, the patient should be evaluated clinically for indicators of hypovolemia or volume overload. The presence of basilar crackles or a third heart sound implies too vigorous fluid replacement, Chapter 10 the Patient with Acute Kidney Injury 233 with resultant cardiopulmonary congestion. Prerenal azotemia on this setting is usually a secondary drawback overshadowed by primary cardiac or liver disease. Ordinarily, however, the management objective is to cut back signs and deal with ascites and edema with a sodium-restricted food plan (1 to 2 g of salt per day), an aldosterone antagonist.
Buy glyset 50 mg fast delivery
The fluid collection has irregular fat-containing borders cheap glyset 50mg overnight delivery, which symbolize the omentum buy generic glyset 50 mg on line. Mild stable wall enhancement is seen alongside the partitions of the gathering glyset 50 mg line, which represents gentle irritation. An oval susceptibility artifact secondary to surgical clips on the dome of the liver is seen. The collection exhibits average wall enhancement, which is suggestive of an infection � abscess. The differential diagnosis of rejection consists of biliary obstruction, cholangitis, ischemic injury, viral an infection, and drug toxicity. These findings could develop secondary to mild ascending cholangitis and medical correlation is required as focal bile duct dilatation with mild irritation (without infection) secondary to postsurgical changes/bile duct ischemia may also be associated with early transient elevated enhancement. The presence of bile duct wall enhancement in the later phases is suggestive of more distinguished inflammation/infection. The intrahepatic biliary ducts reveal multiple diffuse strictures and dilatations on the 3D reconstructed image (f). The frequent bile duct additionally seems diffusely thin, which once more might develop secondary to ischemic modifications and a reasonable stricture is also seen at the anastomosis line (arrows; d�f). The lesion shows progressively reducing enhancement with the event of necrosis. After 3�6 months, responsive lesions become a lot smaller and the enhancement decreases prominently. Unresponsive or partially responsive lesions demonstrate further development over this time period with enhancement. Increased early enhancement of this area, which fades to isointensity/isodensity in later phases, may be seen due to the presence of inflammation secondary to radiation. In successfully handled lesions, mildly elevated thin rim-like enhancement could additionally be seen within the hepatic arterial dominant phase, which tends to turn into isointense/isodense in later phases, because of the presence of peripheral irritation. Recurrent tumors usually show early elevated enhancement or progressively rising enhancement. Treated small metastases could present early peripheral enhancement with progressive centripetal enhancement in later phases, with retention of distinction, at roughly 1 yr following remedy. Good response of metastases is usually reflected by mild early intensity of ring enhancement on the hepatic arterial dominant phase, with progressively intense enhancement of the ring on delayed phases. Treated subcapsular and peripheral lesions may be related to capsular retraction. Fibrotic chronically treated lesions show progressive enhancement, which is extra prominent within the interstitial section. Systemic chemotherapy Responsive lesions present dimension lower beginning 1 month after the beginning of therapy. After the completion of chemotherapy, the lesions demonstrated important lower in measurement and enhancement on the corresponding T2-weighted images (f, g) and postgadolinium T1-weighed images (h, i). After the completion of chemotherapy, the metastases present interval prominent enhance in dimension compared to prior examination, as seen on the corresponding images (d�f), as the metastases are unresponsive to the chemotherapy. The oval lesion exhibits low signal depth on T2-weighted picture (a), isointense to mildly hyperintense sign on T1-weighted image (b) and no enhancement on postgadolinium pictures besides a light peripheral rim kind of enhancement on the hepatic venous part image (d). The peripheral rim sort of enhancement could also be a sign of posttreatment inflammatory response; nevertheless, it should be adopted up. Liver infarction, liver abscess, gallbladder damage, tumor rupture, and liver failure are complications of chemoembolization. Sterile gas may be rarely seen in lesions postchemoembolization remedy, reflecting necrosis and nitrogen launch. Care should be taken to distinguish this from abscess, with the latter often being related to intense hepatic arterial dominant perilesional enhancement and later peripheral rim type of enhancement. Perfusion abnormalities related to the therapy, with increased and heterogeneous enhancement present in hepatic arterial dominant phase photographs, should fade in later phases. After the first week, the ablation site reveals mildly low signal on T2-weighted picture and high signal on T1-weighted precontrast images. Both ablation sites show excessive T1 signal (b, f) due to their high protein content material on T1-weighted precontrast images. The first lesion shows liquefactive necrosis with excessive T2 signal (a) and the second lesion exhibits coagulative necrosis with low T2 sign (e). No enhancement is seen on postgadolinium pictures, suggestive of profitable ablation with out residual illness. The first set of images (a�d) were acquired 3 weeks after the ablation and show an ablation cavity with low T2 (a)/high T1 (b) signal, demonstrating mild thin peripheral rim type of enhancement (arrows; c, d) within the hepatic arterial dominant and hepatic venous phase. The second set of pictures had been acquired 3 months after the ablation and show interval lower in cavity dimension with no peripheral enhancement. Typically, after a successful ablation, a skinny rim of peripheral enhancement is often seen in 1 month, representing early inflammation and granulation tissue. This thin peripheral rim sort of enhancement resolves in 2 months after the ablation and is now not seen. The fluid assortment accommodates bile and a focal hematoma (black arrows; b�d) as well. The focal hematoma exhibits low signal on T2 weighted images (a, b), excessive signal on T1-weighted precontrast picture (c) and no enhancement on the postgadolinium picture (d). Additionally, focal central bile duct dilatation is detected adjoining to the complicated fluid collection secondary to bile duct harm. However, a focal early enhancing area is famous posterior to the ablation website (long arrow, c) and tends to fade within the hepatic venous section (long arrow, d). This focal early enhancement mimics residual/recurrent illness; nevertheless, it develops secondary to the compensatory enhance within the arterial move because of the thrombosis of the segmental branch of the portal vein (short arrows; b, d). This segmental portal vein department situated posterior to the lesion was thrombosed during the ablation procedure and these findings had been steady for greater than a 12 months. Note that gentle focal intrahepatic bile duct dilatation can be seen on the apex of the ablation website on T2-weighted picture (a) secondary to focal delicate bile duct damage. However, some recurrent metastases could present fading within the later phases after treatment. The ablation website (black arrows; a�c) shows high T1 signal on pre and postgadolinium photographs with none enhancement. The recurrent tumor (white arrows; a�c) shows early elevated enhancement (b) and later washout with capsular enhancement (c). The ablation web site is changed by a gentle tissue displaying high T2 signal (a), isointense T1 sign (b), early elevated enhancement (c) and later wash-out (d). However, residual illness displaying early enhancement and later wash-out is seen in the posterior a half of the lesion. They may have a configuration that has been termed the bear claw sample as a result of its radiating, parallel, and jagged appearance. The hematoma reveals heterogeneously elevated T2 signal (a, b) and prominently increased T1 sign (c, d) which represents blood products. Compressed liver parenchyma reveals mildly increased enhancement around the hematoma.
Purchase glyset 50mg with mastercard
Note the presence of expansile enhancing tumor thrombus in the left portal vein (arrow purchase 50mg glyset with amex, f) and its wash-out on the hepatic venous section (arrow discount 50mg glyset, g) buy glyset 50 mg. The coronal postgadolinium picture reveals the tumor thrombus in the primary portal vein and its intrahepatic branches (arrows, h). Note the presence of elevated secondary compensatory arterial enhancement in the right lobe of the liver in the hepatic arterial dominant part (f). The tumor thrombus (thick arrows) reveals early enhancement (a, c) and later wash-out (b, d). Acute-on-chronic hepatitis reveals focal increased transient enhancement in the hepatic arterial dominant phase, but critically, this irregular elevated enhancement fades in later phases. Transient perfusion abnormalities are characterised by focal or segmental elevated transient enhancement within the hepatic arterial dominant part, which fade in later phases. Occurs in younger adults (second and third decade of life) without sex predominance. Macroscopically, at initial presentation the tumor normally seems as a single, massive, well-demarcated mass. The tumor has a lobular architecture with intervening fibrous septa, Hepatocellular carcinoma 179 which can coalesce to type a central stellate scar. The tumor exhibits heterogeneous increased enhancement on the hepatic arterial dominant part and wash-out on later phases with heterogeneous enhancement of central scar, fibrous septa, and pseudocapsule. The central scar sometimes reveals heterogeneous T2 sign as a result of the presence of fibrosis admixed with outstanding vascular tissue and tissue with high fluid content. On postgadolinium fat-suppressed T1-weighted photographs: Diffuse heterogeneous enhancement on the hepatic arterial dominant phase pictures with wash-out in later phases. The giant and irregular central scar, with radiating septa, is present and enhances heterogeneously on delayed part pictures. Peripheral thick ring-like gentle tissue with or with out central necrosis could additionally be current. Early peripheral enhancement with central progressive enhancement on later phases can also be seen. They usually show early peripheral enhancement and later progressive enhancement on postcontrast photographs. The lesions may differ in dimension and enormous lesions measuring more than 5 cm can also be seen. The lesion exhibits heterogeneous predominantly peripheral enhancement (d) which progresses in the later phases (e). Focal areas of hematopoiesis could develop in various places within the body including the liver, spleen, lymph nodes, paravertebral areas, and even the kidneys or pleura. Focal solitary or multiple lesions could additionally be seen within the liver with extramedullary hematopoiesis. The lymphoma reveals low T2 signal as a result of its excessive cellular content and shows gentle enhancement due to its hypovascularity. Variable heterogeneous T2 signal with low T2 sign representing its fibrous stroma may also occasionally be seen. Delayed imaging may present the enhancing central portion, relying on the predominance of fibrosis. Aggressive tumors could present moderately intense diffuse heterogeneous enhancement on instant postcontrast images. Peripheral hypodense/hypointense rim may sometimes be seen on postcontrast pictures. Investigation for a historical past of a primary extrahepatic malignancy is important, in addition to learning the photographs for a main malignancy. The metastasis shows markedly excessive T2 sign (a) and distinguished early enhancement (b) as a outcome of its hypervascularity. Note the presence of nodular enhancing lesions within the vertebral body secondary to multiple myeloma. Hepatoblastoma Hepatoblastoma is the most typical main malignant tumor of the liver in children. Calcifications and hyperdense areas representing hemorrhage on precontrast photographs could also be seen. Focal areas of low sign on T2 and high signal on T1-weighted pictures characterize hemorrhage. On dynamic postgadolinium T1-weighted pictures, they usually present progressive heterogeneous enhancement. Additionally, multiple foci of reasonably enhancing nodular foci are additionally noted in the enlarged spleen. The lesions present early prominent peripheral enhancement which fade in the later section. The largest lesion reveals peripheral low T2 sign, whereas the opposite lesions show delicate to moderate high T2 sign. The images have blurring due to movement artifacts, though noncooperative patient protocol is used. Additionally, the lesion reveals mild wash-out and capsular enhancement within the later part (e). The lesions show markedly excessive T2 sign and intense enhancement, which is peripheral in early phases and progresses centrally in the later phases. These lesions involute by age 12�14 months and are counterparts of cutaneous rapidly involuting hemangioma. The third group contains diffuse lesions largely replacing the liver and leading to massive hepatomegaly and mass effect. They demonstrate peripheral thick rim-like and/or peripheral nodular enhancement with progressive centripedal filling, which has similarities to hemangiomas. Larger lesions might have central necrosis, which is hypoattenuated, or hemorrhage, which is hyperattenuated. On T1-weighted images, they reveal low signal, although central hemorrhage or thrombosis could additionally be seen as central high sign depth areas. Differential Diagnosis: Metastatic neuroblastoma Mesenchymal hamartoma Hepatoblastoma Mesenchymal hamartoma Mesenchymal hamartoma of the liver is the second most common benign liver tumor in children. These lesions are commonly cystic (85%) although strong lesions (15%) may also be seen. The cystic lesions may seem multiloculated and contain multiple small cysts, although giant cysts can also be detected in these lesions. The statement of hemorrhage in smaller hemangioma-like tumors is a clue to the diagnosis. It most commonly impacts kids between 6 and 10 years of age, though it might additionally happen in adults. Angiosarcoma Angiosarcoma is the most typical primary sarcoma arising in the liver, and accounts for 1. The lesion shows very heterogeneous T2 and T1 sign and the presence of low T2 signal and high T1 sign develops due to the presence of hemorrhage. The lesion shows large peripheral nodular enhancement with centripedal progression.
Opuntia (Prickly Pear Cactus). Glyset.
- Dosing considerations for Prickly Pear Cactus.
- Hangover. Taking prickly pear cactus before drinking alcohol might reduce some symptoms of hangover the next day.
- Are there safety concerns?
- What other names is Prickly Pear Cactus known by?
- High blood cholesterol, obesity, colitis, diarrhea, enlarged prostate, and treating infections caused by viruses.
- What is Prickly Pear Cactus?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96848
Buy glyset 50mg mastercard
Tacrolimus has also lowered each the incidence and severity of acute rejection in head-to-head comparisons 50mg glyset visa. One strategy is to preserve goal trough levels of cyclosporine which might be highest (300 ng/mL) in the first month generic glyset 50 mg mastercard, with gradual tapering to a hundred and fifty to 250 ng/mL by 6 months and 50 to 200 ng/mL after 12 months generic glyset 50 mg on line. Similarly, target tacrolimus ranges are 6 to 12 ng/mL within the first month, 5 to 8 ng/mL for months 1 to 5, and four to 7 ng/mL after 6 months. Alternative Regimens the toxicities of corticosteroids and calcineurin inhibitors have led to multiple scientific trials of withdrawal and avoidance methods. Metaanalysis of late steroid withdrawal has been related to acute rejection and graft loss, significantly in African Americans. Calcineurin inhibitor withdrawal/avoidance is another aim as a end result of nephrotoxicity and other unwanted facet effects. It occurs in 20% to 30% of deceased donor transplants but is unusual in residing donor transplants. Acute Rejection Rejection refers to an immunologic response by the recipient to the transplanted organ. Hyperacute rejection is uncommon and is attributable to preformed antibodies against donor antigen, leading to quick graft destruction after perfusion. Accelerated acute rejection usually occurs 2 to 3 days after transplant, and sometimes is an antibody-mediated process that takes place in presensitized patients with prior transplants, transfusions, or pregnancies. Acute mobile rejection is either a T-cell or antibody-mediated response, or a mixture of both, that may happen at any time, but is commonest from 5 to 7 days posttransplant till 4 weeks after transplant, with a gradual lessening of risk within the first 6 months. Therefore, frequent laboratory monitoring and a high index of suspicion are essential to diagnose acute rejection. Acute rejection typically presents as a decrease in kidney operate, as measured by the serum creatinine. However, rejection can happen without discernable modifications in kidney operate, a course of referred to as subclinical rejection. Some facilities carry out routine "protocol biopsies" to consider for subclinical rejection and different graft abnormalities. Current regimens incorporating newer brokers have lowered the incidence of acute rejection in the first year to 15% or lower, have improved 1-year deceased donor allograft survival to approximately 90%, and may be liable for some of the enchancment in long-term outcomes. The prognosis of acute rejection requires an ultrasound-guided kidney biopsy, with application of the Banff standards to grade the severity of rejection or disclose different pathology. Although most acute rejection could be reversed, its prevalence stays a strong predictor of long-term graft survival, most notably antibody-mediated rejection or T-cell rejection involving the large vessels. Recurrent Disease the diagnosis of recurrent disease is guided by the scientific situation and information of which ailments are likely to recur in kidney transplants. Recurrent nephritis might current as proteinuria, nephrotic syndrome, microscopic hematuria, and lack of function. It can be differentiated from other causes (chronic allograft dysfunction, de novo glomerular disease) by kidney biopsy. In the patient who has undergone transplantation, the essential variables are the frequency of recurrence and frequency of graft loss because of recurrence. Alternatively, IgA nephropathy recurs in roughly 50% of recipients, however uncommonly causes graft loss. Systemic lupus erythematosus can also recur microscopically in kidney allografts however not often is clinically important. Glomerular disease was the reason for 30% of all graft loss in a single examine, half of which was because of recurrent illness. Chronic Allograft Damage Despite a major reduction within the incidence of acute rejection during the last several decades, long-term graft survival has improved solely marginally. The commonest cause of graft loss is patient demise with a functioning graft, the majority of which is due to heart problems, and accounts for 278 Chapter 13 the Patient with a Kidney Transplant close to half of all circumstances. The remaining instances of graft loss are as a end result of a variety of each immunologic (chronic rejection) and nonimmunologic. Glomerular pathology can include recurrent primary or de novo disease, the latter often in the type of transplant glomerulopathy. Chronic antibody-mediated graft damage, sometimes in the type of transplant glomerulopathy, is usually as a outcome of medicine nonadherence and has been reported as answerable for over 60% of graft failures. The success of kid- ney transplantation and the growing population of transplant recipients are unfortunately accompanied by the complications from comorbid diseases and unwanted effects of long-term immunosuppression. Patients often die with functioning grafts because of heart problems, infections, and malignancy, and these and different conditions contribute to a spectrum of frequent disorders in transplantation. Infectious Diseases In the patient who has undergone transplantation, typical indicators and signs of an infection may be absent, and coinfections are frequent, necessitating increased scrutiny. Infections after kidney transplantation occur in patterns which are important to acknowledge. Immediately after transplant, patients are in danger for common postoperative infections: wound infections, pneumonia, line, and urinary infections. The first 6 months after transplant is marked by a danger of opportunistic infections as a result of more intense immunosuppression, particularly after antibody induction. After 6 months, the danger of opportunistic infections is lower but stays current, and patients stay in danger for more frequent and extreme infections with community-acquired pathogens. Some widespread pathogens and rules particular to kidney transplantation shall be reviewed. Furthermore, many infections carry an elevated risk of acute rejection due to upregulation of immune surveillance and exercise. In general, mild infections handled with appropriate antimicrobials may be managed with no change in immunosuppression. Severe or life-threatening infections ought to embrace attention to the requirement for stress doses of corticosteroids, which are sometimes sufficient to decrease the danger of rejection throughout an sickness. Reduction of immunosuppression is best done with careful monitoring of graft perform together with the consultation of transplant physicians. Clinically, the disease typically presents as low-grade fever, leukopenia and/or thrombocytopenia, and malaise. Tissue invasion can occur in 5% to 15% of infections, with syndromes of pneumonitis, hepatitis, esophagitis, and diarrhea being most common. Immunohistochemical techniques and the presence of viral inclusions can be utilized to affirm the analysis by way of kidney biopsy. The mainstay of management is 280 Chapter thirteen the Patient with a Kidney Transplant four. For hepatitis B, patients with antigenemia normally receive evaluation and liver biopsy before transplant, as antiviral therapies could additionally be more practical before transplantation. For hepatitis C, the consequences on outcomes and management are considerably controversial. Although many sufferers have mild, indolent illness, there are stories of fast development to cirrhosis and liver failure after kidney transplantation. A complicating factor is that interferon therapy increases the risk of acute rejection. Most patients with hepatitis C should receive liver biopsy to exclude cirrhosis and may have consideration of interferon therapy earlier than transplantation. Protease inhibitors can considerably improve calcineurin inhibitor exposure, and frequent monitoring for applicable dose titration is important when used collectively.
Buy glyset 50 mg cheap
Right-sided pleural effusion and findings of cirrhosis and portal hypertension including ascites discount 50mg glyset overnight delivery, perisplenic/perigastric/peritoneal varices and splenomegaly are detected cheap glyset 50mg free shipping. The tumor is situated in the right lobe of the liver and has mildly increased T2 sign glyset 50mg visa. The tumor shows early elevated heterogeneous enhancement on the hepatic arterial dominant phase (c�e) with wash-out on the hepatic venous section (f). Mild heterogeneous enhancement is seen within the superior a half of the best portal vein, suggestive of tumor thrombus. Note the presence of early transient increased enhancement in the right lobe of the liver, which fades on the hepatic venous section, secondary to compensatory enhance in the hepatic arterial flow. The right portal vein (arrows; a�c) shows early elevated enhancement (a) and wash-out (b, c) within the later phases. The left lobe of the liver is diffusely enlarged with lobulated contours and exhibits decreased T1 sign (a) due to the involvement of tumor. Note that nonocclusive however outstanding thrombus (thin arrow, d) can also be current within the dilated inferior vena cava. Gadolinium in the hepatic arteries is delivered quicker than portal venous and in greater concentration, explaining the transient hepatic arterial dominant increased enhancement. The liver reveals heterogeneous enhancement on postgadolinium pictures with elevated central enhancement significantly involving the caudate lobe within the hepatic arterial dominant part. Mildly elevated central enhancement on the hepatic arterial dominant section and mildly increased enhancement in the periphery on later phases relative to central liver. The liver exhibits heterogeneous enhancement on postgadolinium images with elevated central enhancement particularly involving the caudate lobe. Note the presence of a large quantity of ascites and a few small cysts in the liver. The hepatic vein branches seem thrombosed with related elevated perivenular enhancement (arrows; b, c). Note the presence of delicate heterogeneous enhancement on the left lobe of the liver (asteriks, a). Intrahepatic venous collaterals (arrows; a�c), which develop due to the thrombosis of hepatic veins, drain right into a collateral extrahepatic giant vein (arrows; d, e) which also drains into the inferior vena cava. Early enhancing nodules (arrows; f, h), which are inclined to turn into isointense with the remaining liver within the later phases, can be seen in sufferers with Budd�Chiari syndrome. Hepatic infarction Hepatic infarction is rare because of twin blood supply of the liver including hepatic arterial and portal venous flows. The presence of collateral vessels is another protecting issue towards infarction. Hepatic arterial disease should be present to end in infarction, but often, extra portal venous compromise happens. Hepatic arterial thrombosis/hepatic ischemia � infarction Hepatic ischemia Most commonly seen in the setting of liver transplantation. Other common settings are extreme small vessel disease (such as extreme system lupus erythematosis or eclampsia in pregnancy). These findings are suggestive of hemorrhagic adjustments and decreased perfusion (arrows) secondary to hepatic arterial ischemia. The infarct shows gentle to moderate high T2 sign (a), heterogeneous T1 sign with high sign hemorrhage on T1-weighted image (b) and decreased enhancement on postgadolinium pictures (c, d). However, some heterogeneous enhancement may also be seen on later phases although nonenhancing areas reflecting necrosis, hemorrhage, or fibrosis are often seen. Delayed enhancement of focal areas of parenchyma, which show initial diminished enhancement, typically reflects ischemic somewhat than necrotic hepatic parenchyma, but may at times mirror the presence of vascularized fibrotic tissue (which could be noticed > 1 month after the start of the ischemic process). The vascular fistula between the best portal vein and proper hepatic vein is seen and causes the early filling of the proper hepatic vein on the hepatic arterial dominant phase. Additionally, early enhancing wedge-shaped (black arrow, a) and nodular areas are seen on the hepatic arterial dominant part due to vascular shunting/perfusion abnormalities. Vascular malformations/fistula/aneurysms Primary: Congenital Secondary: Occur secondary to: � Trauma. Fistulas and vascular malformations show enlarged feeding/draining vessels, which may be associated with transient hepatic arterial dominant part focal parenchymal blush. A skinny rim of enhancement may be seen along the resection margins in the hepatic arterial dominant section, which fades to isointensity in later phases. In profitable complete resection, by 6 months postprocedure negligible enhancement is seen in these resection areas on postcontrast pictures. These changes are most prominent within the first 3 months after surgical procedure and progressively lower over the following 6 months. After proper hepatectomy, hypertrophy of the medial section might create the appearance of a pseudo right lobe. A advanced fluid collection with excessive T2 signal is seen alongside the resection margin, which represents a biloma. The blood merchandise present low T2 sign (a) and high T1 (b, c) signal on precontrast pictures. Rarely, gasoline could additionally be seen in areas of hepatic laceration or hematoma within 2 to three days following blunt abdominal trauma, which could be secondary to the trauma itself or as a result of underlying an infection, ischemia, or necrosis. Bile duct injury might lead to collections of bile adjoining to the liver, termed bilomas, or free intraperitoneal leak of bile. Increasing amount of free fluid in the abdomen following liver trauma may characterize intraperitoneal hemorrhage or bile leak. It can be one of the widespread cardiovascular diseases and a serious explanation for stroke in developed international locations, constituting a major public well being downside. It is also more commonly seen in males across all age teams, and in those with cardiovascular disease. If one appears specifically at patients over the age of 65, the admission charges are up to ten fold larger, and this has consistently risen over the past twenty years. In addition, these studies hallmark that the incidence and prevalence is growing rapidly as the developed world struggles to master an weight problems epidemic and as their populations stay longer. This is extra likely to happen in the older affected person with a faster coronary heart rate at admission and those with concomitant coronary heart failure. Prevalence, incidence and lifelong risk of atrial fibrillation: the Rotterdam research. Study of the prevalence of atrial fibrillation normally apply sufferers over sixty five years of age. Estimation of total incremental health care costs in sufferers with atrial fibrillation within the United States. Atrial fibrillation in acute myocardial infarction: a scientific evaluation of the incidence, medical features and prognostic implications. Trends in hospital activity, morbidity and case fatality related to atrial fibrillation in Scotland, 986�996. Significant signs or other proof for notable ischaemia or haemodynamic instability will necessitate this motion, as could pre-excitation with rapid antegrade conduction. Ischaemia, coronary heart failure, or a sign for continuous electrocardiogram monitoring during the first days of remedy are widespread indications for hospitalization.
Purchase glyset 50 mg with visa
Patients were subdivided into three teams: group 1 (urinary calcium excretion greater than 275 mg/day); group 2 a hundred and twenty Chapter 6 the Patient with Kidney Stones (urinary calcium excretion 200 to 275 mg/day); and group 3 (urinary calcium excretion less than 200 mg/day) buy glyset 50mg without prescription. Urinary calcium excretion declined by 29% in group 1 glyset 50mg free shipping, 19% in group 2 50 mg glyset, and 10% in group three. Relative supersaturation of calcium oxalate fell by 12% in group 1 and 6% in group 2, an effect that was statistically significant but less than the fall in urinary calcium. Calcium phosphate relative supersaturation fell in all three groups: 31% in group 1; 22% in group 2; and 17% in group three. These authors recommend that intake of oxalate, sodium, and meat merchandise be limited in all patients with calcium-containing kidney stones. They additionally advocate that sufferers with urinary calcium excretion larger than 275 mg/day be treated with dietary calcium restriction (400 mg/day), thiazide diuretics, and potassium citrate. Patients with urinary calcium excretion between 200 and 275 mg/day are treated with gentle calcium restriction (800 mg/day) and potassium citrate. Those with calcium excretion lower than 200 mg/day are treated with a liberal calcium consumption and potassium citrate. Based on studies mentioned earlier, the function of dietary calcium in the prevention of calcium-containing stones remains controversial. Another research examined the results of the Atkins food plan on threat elements for calcium-containing stone illness. Net acid excretion elevated by 56 mEq/day, urinary citrate decreased from a mean of 763 to 449 mg/day, urinary pH fell from 6. Patients with a history of kidney stones should avoid this extremely lithogenic food plan. The question of whether supplemental calcium will increase threat of nephrolithiasis in women is controversial. One report instructed that any use of supplemental calcium raises the relative risk of stone disease by roughly 20%. Although the relative danger of kidney stone formation is elevated by supplemental calcium, one ought to bear in mind that ladies, in general, are at decrease danger for stone formation. In sufferers with a historical past of calcium-containing stones, urinary calcium excretion, in addition to calcium oxalate and phosphate saturation, must be monitored intently. If saturation will increase, consideration should be given to discontinuing the supplements. Therapy is focused on agents proven to reduce the relative danger of stone formation in randomized placebo-controlled scientific trials with greater than 1 12 months of follow-up (results shown in Table 6-3). This is the results of a minimal of two elements: (a) regression to the imply and (b) increased adherence to nonspecific types of treatment. Trials with less than 12 to 24 months of follow-up must be viewed with skepticism if no impact is detected. At the beginning of therapy, patients at high danger for recurrence could have stones too small to be detected radiographically Chapter 6 the Patient with Kidney Stones 121 that develop and subsequently are identified as new stones. Because calcium-containing stones are often troublesome to stop from growing in size once a nidus is established, this might reduce the remedy impact in high-risk sufferers. Agents that have been proven to be effective in randomized placebo-controlled trials with an extended duration of follow-up embrace thiazide diuretics, allopurinol, potassium citrate, and potassiummagnesium citrate. Thiazides act directly to increase distal calcium reabsorption and not directly to improve calcium reabsorption in the proximal tubule by inducing a state of mild quantity contraction. Volume contraction have to be maintained and hypokalemia prevented for thiazide diuretics to remain maximally efficient. The doses utilized in studies that show an impact are high (25 mg of hydrochlorothiazide twice a day, 25 to 50 mg of chlorthalidone once a day, or 2. Amiloride acts independently of thiazides at a more distal web site and can be added if required. Four randomized controlled trials in recurrent calcium oxalate stone formers demonstrated a reduction in new stone formation threat with thiazide diuretics. Although all patients in these trials had been calcium oxalate stone formers, the minority were really hypercalciuric. This suggests that thiazides might have further results past lowering urinary calcium or that the discount of urinary calcium, even in the absence of hypercalciuria, might scale back the chance of recurrent kidney stone formation. Slow-release impartial phosphate seems to be higher tolerated and may turn out to be the second-line agent of choice. Randomized managed trials of potassium acid phosphate and magnesium hydroxide confirmed no profit in comparison with placebo. Each of these brokers lowered the relative threat of stone formation in randomized controlled trials. Potassiummagnesium citrate may be particularly useful in patients receiving thiazide diuretics, as a end result of potassium and magnesium losses induced by the diuretic are repleted. Citrate preparations are often difficult for patients to tolerate secondary to diarrhea. Slow-release preparations similar to Urocit-K are well tolerated but are relatively expensive. In sufferers with urinary citrate levels less than 150 mg/24 hours, 60 mEq of citrate should be 122 Chapter 6 the Patient with Kidney Stones c. Whether alkalinization is of profit is unclear, because "salting out" can be initiated by sodium urate. Citrate might reduce calcium oxalate precipitation on this setting, but this remains to be proved. Enteric hyperoxaluria ought to be initially treated with a low-fat, low-oxalate food regimen. It stays to be decided if enteral administration of oxalate-degrading bacterium O. This is finest completed by drinking water, which is the one liquid shown to reduce stone formation rate in randomized controlled medical trials. A current research means that even in sufferers with a substantial genetic susceptibility for developing nephrolithiasis, espresso, milk, and maybe tea may also be protecting in opposition to stone formation. This strategy, directed at both specific and nonspecific danger factor reduction, was shown to decrease frequency of recurrent stone formation and cut back the variety of cystoscopies, surgical procedures, and hospitalizations. All randomized controlled trials to date have enrolled patients with either pure calcium oxalate stones or those containing calcium oxalate and a small share of calcium phosphate (<20%). Stones which are predominantly calcium phosphate (60% calcium phosphate salt-usually either brushite or apatite) may be rising in frequency over the last a number of decades. Lowering urinary calcium and growing fluid ingestion seem prudent and are likely beneficial. However, use of potassium citrate which might raise urinary pH could also be dangerous, provided that rises in urinary pH are associated with increases in calcium phosphate supersaturation.
Cheap 50 mg glyset mastercard
Surgical excision of preauricular cysts and sinuses is indicated to forestall secondary infection glyset 50 mg amex. An skilled surgeon should carry out the excision as a end result of the process could also be sophisticated by a number of cysts alongside a tract that ends on the periosteum of the auditory canal purchase glyset 50 mg free shipping. Accessory tragi the tragus is derived from the dorsal portion of the primary branchial arch cheap glyset 50mg. The similar hearing and renal screening recommendations discussed above concerning preauricular pits should be followed. Accessory tragi are often isolated defects, but could also be associated with different developmental abnormalities of the primary branchial arch. Incomplete fusion might result in entrapment of epithelium, forming cysts that talk to the skin surface via sinuses. Lip dimples Cutaneous bronchogenic cysts Thyroglossal duct cysts Midline cervical clefts Diagnosis and remedy the prognosis is usually clinically obvious. Histologically, there are quite a few tiny hair follicles with distinguished connective tissue. Supernumerary digits (rudimentary polydactyly) Supernumerary digits arise from the lateral surface of a traditional digit. They are commonest on the ulnar surface of the fifth digit, however could happen on any finger. These lesions should be surgically excised and the associated nerve dissected if current. Ligating the supernumerary digit with suture materials without utterly eradicating the nerve could end in pores and skin necrosis, an infection, and painful neuromas in grownup life. They are painless, cell, cystic swellings within the neck which will swell throughout respiratory tract infections. Branchial cleft cysts derived from the first branchial arch are very rare and are positioned in the periauricular area or on the upper neck anterior to the sternocleidomastoid muscle. Branchial cysts are lined by stratified squamous epithelium or, hardly ever, by ciliated columnar epithelium. Squamous cell carcinomas arising in these cystic lesions have been described in adults. Branchial cleft anomalies should be surgically excised to forestall infection, with careful consideration to the potential of a true fistula connecting to the tonsillar oropharynx. Preoperative imaging may be necessary to exclude the chance of true fistulae. They result from the persistence of a tract shaped during the migration of the rudimentary thyroid gland from the bottom of the tongue to the anterior cervical regions. The most typical location is on, or just lateral to , the midline neck in the area of the hyoid bone, however they might be found anywhere from the posterior tongue to the suprasternal notch. Most thyroglossal duct cysts current in childhood as an asymptomatic neck mass that moves upward with tongue protrusion or swallowing. Occasionally, ectopic thyroid tissue can be found in these cysts, and an association with thyroid cancer has been reported. The treatment is full surgical excision in order to forestall progress and an infection. Preoperative imaging with high-resolution ultrasound is necessary to confirm the prognosis and determine the presence of a normal thyroid gland. The cyst wall may include clean muscle, mucus glands, and cartilage and lymphatic tissue might or may not be present. The differential prognosis includes branchial arch cysts, thyroglossal duct cysts, teratomas, and heterotopic salivary gland tissue. Median raphe cysts widespread cutaneous location is within the subcutaneous tissue on the suprasternal notch, but different areas embody the lateral neck, scapula, and presternal space. Thus, these cysts must be included in the differential diagnosis of both lateral and midline neck lots. They are asymptomatic, small cystic swellings that may steadily enlarge over time and will discharge a mucoid material. Bronchogenic cysts are lined by lamina propria and a pseudostratified columnar ciliated epithelium with goblet cells. The cysts can occur at any web site on the ventral floor of the male genital region, together with the parameatus, glans penis, penile shaft, scrotum, or perineum. These malformations are the results of incomplete or faulty closure of the neural tube. Cephalocele is the final term for congenital herniation of intracranial structures through a cranial defect. Meningoceles are cephaloceles by which only the meninges and cerebrospinal fluid herniate through a calvarial defect. Large encephaloceles and meningoceles pose no diagnostic drawback and are often easily diagnosed prenatally or at birth. Smaller or atretic encephaloceles and meningoceles may be mistaken for cutaneous lesions corresponding to hematomas, hemangiomas, aplasia cutis, dermoid cysts, or inclusion cysts. These varied classifications have been derived from the amount and kind of neural tissue present, in addition to the diploma of connection to the central nervous system. Therefore, all congenital exophytic scalp nodules should be evaluated completely, as 20�37% of congenital, nontraumatic scalp nodules hook up with the underlying central nervous system. They are normally midline, though they might even be found Cutaneous signs of neural tube dysraphism the skin and the nervous system share a common ectodermal origin. Separation of the neural and cutaneous ectoderm happens early in gestation, at the similar time the neural tube is fusing. This shared embryologic origin explains the simultaneous incidence of congenital malformations of the skin and neural tube dysraphism, which is an incomplete closure or defective fusion. Open neural tube defects are sometimes massive and recognized in utero or at delivery; however, closed or occult neural tube defects often current solely with congenital abnormalities of the pores and skin overlying the defect. It is important to acknowledge these cutaneous markers and display screen with the suitable radiologic imaging techniques. A basic data of embryology and formation and closure of the neural tube is helpful in identifying which cutaneous markers are highly indicative of underlying defects. Small cephaloceles are clinically heterogeneous; their appearance dictated by the sort and amount of cutaneous ectoderm overlying the lesion. They may be covered with regular skin, or have a blue, translucent, or glistening surface. There is often a disruption of the surrounding and overlying regular hair sample. They are gentle, compressible, spherical nodules that enhance in size when the child cries or with a Valsalva maneuver. The association of a congenital scalp mass with other cutaneous abnormalities makes the diagnosis of cranial dysraphism extremely suspicious. All congenital midline scalp nodules carry a significant risk of intracranial connection and should have radiologic imaging studies performed before surgical removing to prevent issues similar to meningitis. Differential analysis and management Included in the differential diagnoses of congenital scalp nodules are pilomatrixoma, epidermoid cyst, lipoma, osteoma, eosinophilic granuloma, hemangioma, sinus pericranii, dermoid cyst, leptomeningeal cyst, and cephalohematoma. Immediate neurosurgical referral is required for surgical removing and reconstruction.
References
- Zoghbi WA, Enriquez-Sarano M, Foster E, et al. Recommendation for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777.
- Demers C, Ginsberg JS, Hirsh J, et al: Thrombosis in antithrombin-III-deficient persons. Report of a large kindred and literature review, Ann Intern Med 116:754, 1992.
- Burda C, Chen X, Narayanan R, et al. Chemistry and properties of nanocrystals of different shapes. Chem Rev 2005;105:1025-102.
- Iversen P, McLeod DG, See WA, et al: Antiandrogen monotherapy in patients with localized or locally advanced prostate cancer: final results from the bicalutamide Early Prostate Cancer programme at a median follow-up of 9.7 years, BJU Int 105(8):1074n1081, 2010.
- Helgadottir A, Thorleifsson G, Magnusson KP, et al: The same sequence variant on 9p21 associates with myocardial infarction, abdominal aortic aneurysm and intracranial aneurysm, Nat Genet 40(2):217-224, 2008.
- Singh SM, Wann LS, Schuchard GH, et al: Right ventricular and right atrial collapse in patients with cardiac tamponadeóa combined echocardiographic and hemodynamic study, Circulation 70:966, 1984.