
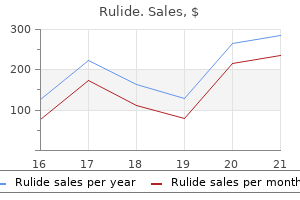
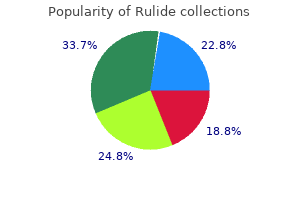
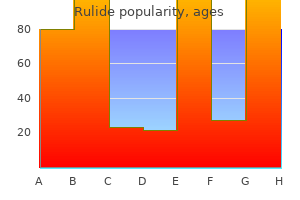
Rulide
Marie Adorno, APRNC, MN
- Associate Professor of Nursing
- Our Lady of Holy Cross College
- New Orleans, Louisiana
Rulide dosages: 150 mg
Rulide packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy rulide 150 mg otc
Primary syphilis is characterized by a nontender treatment 20 cheap rulide 150mg, pink symptoms 7 days after implantation discount 150 mg rulide amex, round treatment 5th metatarsal base fracture 150 mg rulide, agency ulcer approximately 1 cm in dimension with raised edges, generally recognized as a chancre. The vesicles described on this case are totally different than that sometimes seen in main syphilis. The lesion presents initially as an erythematous papule, which evolves to a pustule and ulcer. The ulcer is painful with an erythematous base and irregular, well-demarcated borders. Vignette 3 Question 2 Answer D: A definitive analysis of genital herpes ought to be made through viral or serology testing. On the opposite hand, empiric remedy of chlamydial an infection is beneficial in sufferers contaminated with N. It is commonly a polymicrobial infection with a big selection of pathogens, including skin and gastrointestinal flora in addition to the usual flora colonizing the lower reproductive tract. Mycobacterium tuberculosis is a uncommon reason for persistent endometritis in developed international locations however is a number one cause of infertility in endemic countries. Chronic endometritis could be suspected in sufferers with persistent irregular bleeding, discharge, and pelvic pain. The prognosis can be made in a nonpuerperal affected person with endometrial biopsy showing plasma cells. This can result in ascending infections of the uterus, fallopian tubes, adnexa, pelvis, and abdomen. In nonpuerperal infections where chlamydial infection may be the suspected cause, doxycycline should be added to the regimen for a complete of 14 days. It is seen most commonly after cesarean delivery, but also after vaginal deliveries and surgical pregnancy terminations. However, antibiotic prophylaxis is really helpful for cesarean sections, surgical terminations of pregnancy, and hysterosalpingography or sonohysterography in girls with a history of pelvic an infection or if dilated tubes are demonstrated. Additionally, the risk of ectopic pregnancy is elevated as much as 7- to 10-fold and approximately 20% of ladies develop chronic pelvic ache throughout their lifetime. Sequelae, together with chronic pelvic ache, dyspareunia, and pelvic adhesions, can also require surgical therapy, contributing to the economic costs and morbidity of this illness. Among sexually lively ladies, the incidence of this illness is highest in the 15- to 25-year-old age group (at least three Chapter 17 / Upper Female Reproductive Tract and Systemic Infections times greater than in the 25- to 29-year-old age group). The character of the ache can vary (burning, cramping, stabbing) and can be unilateral or bilateral. Other associated signs embody elevated vaginal discharge, irregular odor, abnormal bleeding, gastrointestinal disturbances, and urinary tract signs. Typically, a repeat pelvic examination is carried out after the patient has been afebrile for twenty-four to 48 hours to monitor for improvement and eventual decision of tenderness. If conscious of medical management, the patient can be transformed to oral antibiotics to complete a 10- to 14-day course with doxycycline plus clindamycin or metronidazole. Most sufferers will endorse belly and/or pelvic pain (90%) and reveal fever and leukocytosis (60% to 80%). Culdocentesis that reveals gross pus is diagnostic however has been used less as advances in imaging studies have been made. Finally, laparoscopy can lead to a definitive diagnosis however is often used only when the scientific picture is unclear. Since 1984, the incidence has decreased dramatically and the present annual incidence is estimated at 1 to 2:a hundred,000 women. Blood cultures are sometimes adverse, probably as a end result of the exotoxin is absorbed via the vaginal mucosa. Unless the abscess is ruptured and inflicting peritoneal signs or is impenetrable by antibiotics, surgical remedy can typically be avoided. Clindamycin (900 mg every eight hours) plus gentamicin (loading dose of 2 mg/kg, followed by 1. For more severe cases during which sufferers are hemodynamically unstable, admission to an intensive care unit may be essential. However, it does lower the risk of recurrence, which has been as excessive as 30% in women who continued to use high-absorbency tampons. Antibiotic therapy consists of clindamycin plus Chapter 17 / Upper Female Reproductive Tract and Systemic Infections vancomycin for empiric treatment when particular S. The approach to this illness is prevention of transmission, prophylaxis of opportunistic infections, and prolonging the lives of infected patients by slowing development of illness with antiretroviral brokers. Delaying the progress of the illness is accomplished primarily with nucleoside analogs and protease inhibitors. Second, the high incidence of invasive cervical most cancers on this inhabitants requires more aggressive screening than in the common population. Increased transmission could be seen with higher viral burden or advanced illness within the mother, rupture of the membranes, and invasive procedures throughout labor and supply that increase neonatal publicity to maternal blood. Vertical transmission can occur intrauterine (20% to 50%), intrapartum (50% to 80%), or postpartum (15%). Initially, the an infection is totally asymptomatic, although the person is a carrier of the disease; this stage can final from 5 to 7 years. This test does have false-positive results, which, in low-risk populations, may occur more often than true constructive results. Another level of affirmation may be obtained if a viral load is shipped and is constructive. The Centers for Disease Control and Prevention presently recommends routine Pap smears at preliminary analysis and 6 months later. Cesarean delivery has been proven to decrease transmission rates by roughly two-thirds in comparison with vaginal delivery in sufferers on no therapy and notably without onset of labor or rupture of membranes or in the setting of excessive viral load. Vertical transmission charges throughout being pregnant have been proven to decrease with antiretroviral remedy and are positively related to viral load. Examination reveals a gentle abdomen and lower quadrant tenderness without guarding or rebound. None of the above A 28-year-old G1P1 presents to the emergency division 4 days after main cesarean section with complaints of fever, malaise, and increased decrease belly pain for the past 6 hours. Her labor course was difficult by prolonged rupture of membranes and stage 2 arrest because of cephalopelvic disproportion leading to a cesarean supply. Her postoperative course was uncomplicated and he or she had been discharged house stable the day previous to presentation. Low socioeconomic standing Vignette 2 A 20-year-old nulligravid younger girl presents to the emergency department four hours after the onset of nausea, vomiting, and reasonable decrease stomach pain. She reviews three new sexual partners within the last 6 months and makes use of condoms intermittently. On examination, her stomach is diffusely tender with guarding and rebound present. On vaginal examination, her cervix is dilated to 6 cm with a bulging bag of water. None of the above Vignette four A 34-year-old G2P2 girl comes to the emergency division with 8 hours of accelerating proper decrease quadrant pain, incapability to tolerate orals, and nausea.
Order 150 mg rulide with visa
This is facilitated by steadily flexing and externally rotating the adducted humerus medications 7 rights buy generic rulide 150mg online. This permits identification of the anatomic neck and the peripheral extent of the native articular surface treatment 1st degree burn purchase 150 mg rulide overnight delivery. The humerus is delivered into the wound with simultaneous adduction medicine 7 year program order 150 mg rulide mastercard, extension, and external rotation in this right shoulder. Retractors embody a Brown deltoid retractor superiorly, a large Darrach retractor medially, and a blunt Hohmann retractor anteroinferiorly on the calcar. Accurate placement of the central guide pin is an important portion of the resurfacing procedure. This guide pin fixes the middle and inclination of the articular floor in all planes. Once the guide pin is anatomically positioned, the rest of the process is only a matter of selecting the appropriately sized head and putting it on the acceptable depth. Reaming proceeds over a centrally placed guidewire till the highest of the humeral head is flattened fully. The excess bone is faraway from the periphery to produce a flat shelf on which the component can be seated. The guides usually are hemispherical and cannulated centrally so that the sting of the information is positioned parallel to the articular margin within the visual heart of the pinnacle. Once the surgeon is glad with pin placement, shaping of the humeral head to match the deep surface of the resurfacing implant can start. Reamers are chosen primarily based on the anticipated measurement of the prosthetic humeral head, which is, in flip, determined via a mix of preoperative templating and intraoperative measurements. Reaming can proceed to inside 2 to 3 mm of the rotator cuff reflection superiorly. The central punch is placed over the guide pin and driven into the humeral metaphysis to put together it for the central peg of the prosthetic head. This requires removal of extra bone from around the periphery of the projected seating level of the implant. Two small bone anchors are placed within the humerus medial to the osteotomy but lateral to the humeral prosthetic edge. The sutures on the anchors are handed in a mattress configuration through the subscapularis tendon from deep to superficial at the bone�tendon junction. With the humerus reduced and the arm in neutral rotation, the deep limbs of the three sutures beforehand passed around the lesser tuberosity are handed via the cancellous bone of the osteotomy mattress as far laterally Glenoid Inspection, Capsular Excision, and Release the information pin is eliminated and the glenoid is uncovered by putting a humeral head retractor inside the joint and retracting the humeral head posteriorly. The clamps on these three sutures are pulled laterally to maintain the lesser tuberosity in a decreased place. After the rotator interval suture is tied, the three interfragmentary sutures are tied, adopted by the sutures from the anchors. Passive movement achievable with out undue tension on the subscapularis restore is noted for guidance of postoperative rehabilitation. The wound is closed in layers with interrupted absorbable sutures in the subcutaneous tissues and a running subcuticular monofilament suture. The methods of superficial and deep dissection, lesser tuberosity osteotomy, capsular launch, and osteophyte excision are the same as described previously. This may be accomplished freehand or with intramedullary or extramedullary guides. Retroversion of the cut in my follow is prescribed by the plane of the periphery of the native articular surface (ie, native retroversion). A the neck�shaft angle of the humeral minimize is decided by the sort of implant used. With fastened neck�shaft angle gadgets, the minimize should precisely match the neck�shaft angle of the chosen device. Preoperative templating ought to establish the patient with an extreme varus (less than 125) or valgus (greater than a hundred forty five degrees) neck�shaft angle. The reduce exits superiorly 2 to 3 mm medial to the cuff reflection and inferiorly via the native head. This will leave a small portion of the native head in place, even after the inferior osteophyte is removed. The reduce exits inferiorly on the native articular margin and superiorly by way of the native head. Alternatively, the minimize could be made alongside the native neck�shaft angle and a variable neck�shaft angle device can be utilized to match the native neck�shaft angle. The measurement of the humeral head is estimated by putting trial humeral heads on the cut surface of the osteotomy. After removing of all osteophytes, the placement of the anatomic neck is marked with an electrocautery. The humerus is reduce in native retroversion, leaving 2 to 3 mm of bone medial to the supraspinatus insertion. With the humeral head resected, a Fukuda ring retractor is positioned within the joint and the humerus is retracted posteriorly. A reverse, double-pronged Bankart retractor is placed on the scapular neck anteriorly, between the anterior capsule and the subscapularis. A blunt Hohmann retractor is positioned alongside the anteroinferior portion of the scapular neck to retract and defend the axillary nerve, and the anterior and inferior capsule is excised. The labrum is excised circumferentially to expose the complete periphery of the glenoid. If greater than 25% posterior humeral subluxation was current preoperatively, care is taken to preserve the posterior capsular attachment to the glenoid. The previously estimated humeral head size could give some idea of the glenoid measurement. The center of the glenoid is marked and a centering drill gap for the glenoid reamer is drilled. The orientation of this drill gap must be perpendicular to the estimated reamed floor. A nonabsorbable suture is handed around the neck of the prosthesis and the prosthesis is impacted into the humerus with the 2 ends of the suture protruding anteriorly. Lesser Tuberosity Repair Humeral Preparation and Component Placement the humerus is redelivered into the wound and the humeral canal is reamed with sequentially larger reamers till mild purchase is obtained within the intramedullary canal. A field osteotome that corresponds to the final reamer dimension is passed into the humerus to cut the footprint of the humeral implant. A broach that corresponds to the dimensions of the box osteotome and ultimate canal reamer is positioned to the appropriate depth. Therefore, a collar is screwed into the broach that creates a 135-degree neck�shaft angle. The 135-degree collar is removed and a trial ball taper fitted with a humeral head trial is inserted into the broach. The trial head and ball taper are positioned into the position that provides symmetrical coverage of the humeral metaphysis, and the taper is locked to the broach.
Purchase rulide 150mg with amex
Approaches to the shoulder that could be used include the deltopectoral medications removed by dialysis rulide 150mg otc, the concealed axillary incision symptoms schizophrenia order 150mg rulide free shipping, and the miniincision method medicine video buy generic rulide 150 mg on line. A 7- to 15-cm incision is made lateral to the coracoid process beginning beneath the clavicle and increasing toward the anterior humeral shaft on the deltoid insertion. This incision is cosmetically appealing and is helpful in sufferers where cosmesis is necessary. The location of this incision is important to obtain direct access to the glenoid with out extending the incision: one third of the incision must be above and two thirds under the coracoid process. The cephalic vein is taken laterally with the deltoid muscle, and the clavipectoral fascia overlying the subscapularis tendon and strap muscular tissues is uncovered. Great care must be taken not to injure the biceps tendon, which lies just beneath the pectoralis main insertion. The clavipectoral fascia is incised lateral to the strap muscular tissues, and a retractor is placed between them to expose the subscapularis muscle and tendon. The branches of the anterior circumflex humeral vessels on the inferior margin of the subscapularis muscle must be cauterized at this time to management bleeding. The subscapularis tendon is exposed and incised vertically just medial to its insertion. Transosseous sutures are handed through holes made with pointed forceps or a drill. Alternatively, suture anchors could also be placed at the margin of remaining articular cartilage. Typically, an inferior capsular shift procedure is carried out together with the Bankart procedure as described beneath. The anterolateral leading edge of the coracoacromial ligament (indicated by the clamp) is resected for improved superior publicity. The subscapularis is incised about 1 cm medial to its insertion, leaving a stout cuff of tissue laterally (arrow) for subsequent restore. The capsule is sharply incised, taking care not to damage the humeral head cartilage below. The method is similar as within the Bankart process described and entails dissection of the subscapularis from the anterior glenohumeral capsule. Unlike the inferior capsular shift process, the T-plasty involves a medially based capsular incision on the glenoid margin. The laterally primarily based inferior flap of capsule is advanced superiorly and medially and secured to the glenoid rim. The T capsulotomy is made two thirds from the highest of the capsule, with the vertical element adjacent to the glenoid rim. A deltopectoral strategy to the shoulder is used and the strap muscles are retracted medially to expose the subscapularis tendon. A horizontal capsulotomy is now made in the course of the capsule extending medial to the glenoid rim. The subscapularis is divided horizontally according to its fibers at the junction of the higher two thirds and decrease one third. The capsule is elevated off the glenoid subperiosteally to enable for superior and inferior capsular advancement. The laterally based mostly inferior flap is shifted superiorly and secured to the intra-articular portion of the glenoid rim utilizing transosseous sutures to attempt to recreate the labral "bumper. The process was designed to treat involuntary inferior and multidirectional instability of the shoulder that could not be addressed by repair of the anterior glenoid labrum alone (the Bankart procedure). The subscapularis tendon is incised about 1 to 2 cm medial to its insertion at the lesser tuberosity, leaving an adequate cuff of tissue for repair. The subscapularis consists of both a superior tendinous portion (two thirds) and inferior muscular (one third) portion. The arm must be ready of adduction and exterior rotation during this inferior dissection, and great care is taken to shield the axillary nerve. By putting traction on the capsular tag sutures in a superior and lateral course, the axillary pouch must be obliterated when an enough quantity of capsular dissection has been carried out. It is important to launch the inferior capsular attachments to the humerus, which have a broad insertion inferior to the articular floor. The medial insertion of the glenohumeral ligaments and glenoid labrum ought to then be assessed for avulsion or tear. Once secure fixation to bone is achieved, the capsule is shifted superiorly and laterally and the nonabsorbable sutures are passed by way of the capsule from an intraarticular to extra-articular location. A bimanual method can be used by which one needle driver is used to cross the suture and a second to "catch" the needle on the extra-articular side. The sutures are then tied on the extra-articular facet to safe the capsule to the glenoid rim. In the inferior capsule shift process, the laterally based mostly capsular incision is sustained inferiorly utilizing tag stitches on the released anterior capsule to apply traction. Release of the dual inferior capsular attachment, permitting an entire shift of the capsule. An anterior crimping (barrel) stitch is used to decrease the redundancy of the anteroinferior capsule. Once tied, the barrel stitch reduces anterior medial capsular redundancy and an anterior inferior bolster is created. The anteroinferior capsule is superior superiorly and reattached to the capsular sleeve preserved on the humeral neck. The superior flap is sewn to the inferior flap to scale back volume and increase strength. The rotator interval capsule is palpated between the subscapularis and supraspinatus tendons. Once the medial instability restore is complete, attention is directed to lateral repair of the capsule to the remaining cuff of tissue at the humeral neck. A good general guideline is to repair the shifted anterior capsule with the arm in 20 levels of abduction and 30 degrees of exterior rotation. Excess tightening of the anterior capsule must be prevented to prevent the event of postcapsulorrhaphy arthropathy. In these shoulders, the capsular incision may be converted to a laterally based mostly T capsulorrhaphy by incising the capsule between the inferior and center glenohumeral ligaments all the method down to the glenoid rim. The inferior limb of the capsule is first repaired to its lateral insertion on the humerus. This will each cut back capsular volume and reinforce the anterior capsuloligamentous tissues. If the rotator interval is widened or attenuated, it should be imbricated and closed utilizing interrupted nonabsorbable sutures.
150mg rulide mastercard
Short-term outcomes after surgical treatment of traumatic posterior sternoclavicular fracturedislocations in youngsters and adolescents medications quizzes for nurses cheap 150 mg rulide amex. Conservative management of a displaced medial clavicular physeal injury in an adolescent athlete medicine 44291 discount rulide 150mg on-line. Chapter 13 Medial Clavicle Excision and Sternoclavicular Joint Reconstruction John E treatment 3 antifungal rulide 150 mg sale. Other circumstances include rheumatoid arthritis, seronegative spondyloarthropathies, crystal deposition illness, sternoclavicular hyperostosis, condensing osteitis, and avascular necrosis. When suspected, the sternoclavicular joint must be aspirated for culture, Gram stain, and cell counts after which handled with irrigation and d�bridement. Traumatic instability is defined by the direction of displacement of the clavicular head and is superior, anterior, or posterior. Posterior instability has been associated with a wide range of probably deadly comorbidities. Atraumatic instability is often anterior and is commonly seen in folks with generalized ligamentous laxity. Symptomatic traumatic instability is best handled with closed reduction and potential reconstruction of the joint, not resection of the clavicle head. The clavicle pivots over the primary rib, dislocating the pinnacle of the clavicle posteriorly. Direct blows to the sternoclavicular joint can even dislocate the clavicle head posteriorly. This is particularly true with the pain and swelling seen in perimenopausal women. Infection could current with a comparatively benign clinical image however will progress and should become serious. It is rare for the sternoclavicular joint to be the primary joint involved in rheumatologic conditions or crystal deposition illness. Important ligamentous restraints to motion embrace the anterior capsule (restrains anterior and posterior translation), the posterior capsule (restrains posterior translation),10 and the costoclavicular ligament (which is the pivot level for movement within the axial plane). Osteoarthritis is most commonly seen in male laborers, in women within the perimenopausal years, and after radical neck dissection. Rheumatologic disorders can have an effect on the sternoclavicular joint as a half of the systemic disease. Other atraumatic situations are much less frequent and the pathogenesis is essentially unknown. The clavicle pivots over the primary rib, forcing the head of the clavicle anteriorly. Traumatic instability might result from high-energy accidents (eg, motor vehicle collision) or could additionally be related to contact in athletics. Posterior instability could additionally be life-threatening because the clavicular head may compress vascular buildings, the trachea, or the esophagus. Atraumatic instability could have an insidious onset and is often related to other signs of generalized ligamentous laxity (eg, patellar subluxation, glenohumeral subluxation). Arteriography must be thought-about in posterior dislocations if vascular injury is suspected. Osteoarthritis, rheumatoid arthritis, seronegative spondyloarthropathies, and sternoclavicular hyperostosis are typically bilateral, with delicate pain, and rare erythema. Traumatic problems With acute traumatic injuries, patients may have vital ache and shall be unwilling to increase the arm. They may describe problem with swallowing or breathing in posterior dislocations. Physical examination is most likely not helpful in figuring out if the instability is anterior or posterior. When infection is suspected, surgeons ought to carry out incision and drainage shortly to forestall late osteomyelitis. Contraindications for resection of the medial clavicle embrace atraumatic instability of the joint. In posterior dislocations, open discount and attainable reconstruction of the joint is indicated if closed reduction fails. The ipsilateral hand is ready and draped as nicely if the surgeon needs to use palmaris as an interposition graft. For reconstructions of the sternoclavicular joint, an ipsilateral hamstring may be used; as such, the knee should be prepared and draped. Preoperative Planning Due to the vital buildings that lie behind the sternoclavicular joint, it is necessary to have a thoracic surgeon obtainable ought to problems develop. Care is taken to defend necessary structures throughout dissection, significantly the origin of the sternocleidomastoid muscle and the costoclavicular ligament. A self-retaining retractor is placed on the capsule, a blunt retractor is positioned subsequent to the articular floor, and a small oscillating noticed is used to take away between zero. Alternatively, the palmaris can be used to augment a reconstruction of an unstable sternoclavicular joint by passing it across the clavicle and first rib (see below). Drill holes are in manubrium with safety of mediastinal buildings with an Army-Navy retractor. Sternoclavicular joint reconstruction for anterior and posterior sternoclavicular joint instability. The surgeon must at all times be diligent for an infection, which can have a comparatively benign appearance. Removing bone Great care have to be taken to keep away from perforating the posterior capsule and entering the mediastinum. Preserving the clavicular head is essential for reconstructions of unstable sternoclavicular joints. Preserving capsule Costoclavicular ligament General surgery Maintaining the integrity of the joint capsule is of crucial significance. If the capsule is stripped fully off the clavicle, suture anchors within the clavicle might help restore stability. If the costoclavicular ligament is sacrificed, the intra-articular disc and disc ligament may be handed into the intramedullary canal. It is sensible to have a thoracic surgeon available ought to issues develop in the mediastinum. Patients put on a sling with pillow help to support the arm when upright for 6 weeks. Patients are instructed to avoid shifting the arm for six weeks to allow for capsular healing and preventing instability. Rockwood and colleagues9 reported that outcomes had been improved if the costoclavicular ligament remained intact (eight of eight wonderful with complete satisfaction). If the costoclavicular ligament was disrupted, nevertheless, the outcomes have been less predictable (three of 5 excellent). Sixty percent were graded nearly as good to excellent, and 93% had important ache reduction and would have the process again.
Order rulide 150mg mastercard
Chapter 34 Open Reduction and Internal Fixation of Capitellum and Capitellar�Trochlear Shear Fractures Asif M symptoms tuberculosis rulide 150mg low price. The anterior side of the lateral column is covered with articular cartilage medications keppra generic rulide 150 mg fast delivery, forming the capitellum medications jaundice purchase rulide 150 mg online. Distally, these two condyles may be visualized as forming a triangle on the end of the humerus. The capitellum is directed distally and anteriorly at an angle of 30 degrees to the long axis of the humerus. The radial head rotates on the anterior floor of the capitellum in elbow flexion and articulates with its inferior surface in elbow extension. The lateral collateral ligament inserts subsequent to the lateral margin of the capitellum. It arises from the lateral arcade, which is the anastomosis of the radial collateral arteries of the profunda brachii and the radial recurrent artery. Capitellar�trochlear shear fractures contain impaction of the radial head towards the lateral column of the distal humerus in a semi-extended place, resulting in a shearing mechanism of the distal humerus. Fracture fragments differ in size and displace superiorly and anteriorly into the radial fossa, leading to impingement with elbow flexion. Capitellar fractures are extra frequent in females, a discovering that has been attributed to the upper carrying angle of the elbow. Elderly sufferers of each genders are extra susceptible to capitellum and complex capitellar�trochlear shear fractures due to the metabolic susceptibilities of osteoporosis. Displaced fractures that go untreated can have a poor end result owing to progressive loss of motion and posttraumatic arthrosis. Although there may be variable lack of forearm rotation, loss of flexion and extension is common, usually accompanied by crepitus and ache. The affiliation of concomitant radial head fractures and ligamentous injuries with capitellar fractures is excessive. Closed reduction strategies, which have been described in the literature, must be carried out with caution, and only full anatomic discount must be accepted. Lateral radiographs are greatest for acquiring an initial analysis of capitellar fractures. This view is a lateral oblique projection taken with the x-ray beam pointing forty five levels dorsoventrally, thereby eliminating the ulno- and radiohumeral articulation shadows. Type 2 fractures are harder to diagnose, relying on the amount of subchondral bone accompanying the articular fragment. Capitellar fractures are unusual, and the big selection of therapy options introduced in the literature relies on comparatively small series. In elderly patients, we do contemplate total elbow arthroplasty for complex intra-articular distal humerus fractures. Characteristic "double arc" signal on lateral radiographs of coronal shear fractures. Fractures ideally should be approached within 2 weeks, before osseous healing units in, but after swelling has gone down. An picture intensifier must be used during surgery to affirm reduction of the fracture and proper positioning of implanted hardware. Approach Either a lateral or posterior midline incision ought to be used, depending on the character of the fracture, adopted by a lateral method into the elbow joint. We advocate the K�cher approach, which uses the interval between the extensor carpi ulnaris and the anconeus and affords greater protection of the posterior interosseous nerve. This could be exploited and used as the interval to expose the fracture, thereby avoiding the necessity to trigger an extra soft tissue defect. The affected person usually is positioned supine on the operating desk, with a radiolucent hand desk. Alternatively, a lateral or prone place can be thought-about, with the anterior surface of the elbow supported by a padded bolster to use the universal posterior method. The frequent extensor origin is sharply raised off the lateral epicondyle and reflected anteriorly to expose the lateral elbow joint. Care should be taken to keep away from injury to the radial nerve touring between the brachialis and brachioradialis. Often the lateral ligamentous complex might be avulsed from the distal facet of the humerus, with or without some facet of the lateral epicondyle. This ligamentous violation may be exploited to improve publicity by hinging open the joint on the medial collateral ligament with a varus stress. The capitellar fracture often is displaced proximally and rotated and has no soft tissue attachments. Reduction and Fixation the fragment is reduced under direct visualization, held with reduction tenaculums, and provisionally fixed with zero. Cancellous screws are finest for fracture fragments with a big subchondral element, as in type 1 fracture fragments. Unrestricted forearm rotation and elbow flexion� extension with out mechanical block or catching should be confirmed intraoperatively. If the lateral collateral ligament is discovered to be avulsed, it ought to be repaired again to the lateral epicondyle with drill holes and nonabsorbable no. The retracted extensor origin should be relaxed and closed to the encompassing soft tissue. In many circumstances, the lateral epicondyle will have avulsed off of the distal humerus, and this traumatic osteotomy may be exploited. Otherwise, a formal lateral epicondyle osteotomy may be carried out to improve visualization whereas maintaining the integrity of the lateral ligamentous advanced. Additionally, an olecranon osteotomy could also be carried out to improve visualization and fixation of fractures extending medially and posteriorly. Inability to cut back the fracture anatomically may represent fracture impaction, requiring either disimpaction or bone grafting, or both. Cancellous screws are finest when the fracture fragment has a big subchondral part, however they make it necessary to extend the dissection posteriorly across the lateral column, theoretically increasing the danger of osteonecrosis. Headless compression screws, such because the Herbert screw, are finest for fragments with less subchondral bone and supply the extra advantage that they can be used in either path, anteriorly or posteriorly. Diligence should be maintained to verify that the pinnacle of the screw is buried under the articular surface when placed anteriorly. Fragment discount and hardware place ought to be confirmed by picture intensifier. Unrestricted forearm rotation and elbow flexion�extension without mechanical block or catching ought to be confirmed intraoperatively. The interval and launched extensor origin ought to be relaxed and closed to the encompassing gentle tissue.
Bastard Cinnamon (Cassia Cinnamon). Rulide.
- What is Cassia Cinnamon?
- Are there safety concerns?
- Diabetes.
- Loss of appetite, muscle and stomach spasms, bloating, intestinal gas, vomiting, diarrhea, common cold, impotence, bed wetting, menstrual complaints, chest pain, high blood pressure, kidney problems, cancer, and other conditions.
- Are there any interactions with medications?
- How does Cassia Cinnamon work?
- Dosing considerations for Cassia Cinnamon.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96963
Purchase rulide 150mg on-line
This may also forestall placement of the osteotomy throughout the first tarsometatarsal joint translational medicine cheap rulide 150 mg otc. The noticed blade is stored parallel to the weight-bearing floor of the foot to forestall undesirable dorsal angulation of the first metatarsal head after completion of the osteotomy medications vaginal dryness buy rulide 150 mg fast delivery. To preserve full management of the osteotomy medications prednisone trusted 150 mg rulide, a guidewire for the cannulated screw can be placed perpendicular within the accomplished proximal portion of the osteotomy. The osteotomy could be completed dorsal-distally without worry of dropping the orientation. Placing a screw too distal might trigger fracture of the dorsal portion of the osteotomy web site. Allow sufficient house between the screws and the distal side of the osteotomy to stop fracture. If encountered, the fist tarsometatarsal joint may be quickly pinned and permanent fixation positioned. The pin throughout the primary tarsometatarsal joint can be removed 4 to 6 weeks postoperatively. Two weeks after surgery the sutures are eliminated and the affected person is fully weight bearing in a surgical shoe. The Mau is a steady osteotomy due to the dorsal shelf to assist cut back dorsal displacement forces and broad bony apposition to facilitate twoscrew fixation. The authors performed a follow-up research evaluating the Mau and crescentic osteotomies. Complications included dorsal malunion, placement of screws throughout the tarsometatarsal joint, and nonunion. This may be because of selection of the inappropriate procedure to right the moderate to extreme bunion deformity or intraoperative failure to get hold of an enough alignment to correct the deformity. It occurs as a outcome of overcorrection of the deformity and is much more tough to correct. Other complications embody shortening, dorsal malunion, and switch lesions, which can occur with all proximal osteotomies. Mechanical comparability of cyclic loading in five different first metatarsal shaft osteotomies. Early outcomes of the Mau osteotomy for correction of average to severe hallux valgus. Relationship of hallux abductus angle and first metatarsal angle to severity of pronation. Conclusions drawn from a comparative examine of the feet of barefooted and shoe-wearing peoples. Hallux valgus repair using a distal gentle tissue process and proximal metatarsal osteotomy: a long-term follow-up. The relationship of irregular foot pronation to hallux abducto valgus, a pilot examine. A study of the correlation between neutral calcaneal stance place and relaxed calcaneal stance position in the development of hallux abducto valgus. Pins present little inherent stability and have been related to postoperative infections. Recently, the utilization of locking plates and locking screws has been rising within the orthopaedic world. The locking plates provide a fixed-angle system, which allows for a doubtlessly stronger method of fixation. Although many alternative configurations of the osteotomy can be used, the proximal chevron osteotomy permits a higher diploma of correction in contrast with distal osteotomies. It does this by way of both an angular and translational displacement of the distal portion of the first metatarsal. A dorsomedial incision is made within the capsule parallel to the primary metatarsal, creating a plantarly based capsular flap with exposure of the medial eminence. First use a blunt Freer elevator to develop some room after which reduce the capsular tissue with a pointy no. The proximal first metatarsal is subsequently exposed each dorsally and plantarly. A plantar and proximally primarily based capsular flap is created, and the capsule is launched with a Freer elevator. A proximally based chevron osteotomy is created at an angle of about 60 levels utilizing a microsagittal saw. The proximal fragment is grasped with a towel clamp, and the distal fragment angulated laterally. The outstanding proximal fragment is cleaned of periosteum and removed flush with the distal fragment. The opening created by plantar flexing the metatarsal creates a gap into which the eliminated bone may be impacted. Correction of the hallux valgus angle and the 1�2 intermetatarsal angle is confirmed with fluoroscopy. During the strategy, dissect thick tissue flaps to allow for improved wound healing. Pay explicit consideration to maintaining the saw in the same airplane while performing the proximal chevron osteotomy to guarantee good bony apposition at the website of fixation. Do not overcorrect the 1�2 metatarsal angle; a adverse angle will cause hallux varus. By eradicating redundant medial capsule in the course of the strategy, the capsule restore may be completed extra efficiently at the conclusion of the process. The nice toe ought to be positioned in slight varus, about 2 levels, to allow healing of the capsular tissues in a great place. Do not overtighten the capsule, as a end result of this will overcorrect the toe place and lead to varus malalignment. Capsular imbrication also can be utilized to right pronation deformity of the hallux. Heel weight bearing could be allowed immediately postoperatively, with advancement to weight bearing as tolerated in an everyday shoe at 6 weeks postoperatively. Prospective, randomized comparability of proximal crescentic and proximal chevron osteotomies for correction of hallux valgus deformity. Bunion surgical procedure using locking-plate fixation of proximal metatarsal chevron osteotomies. Comparison of stability of proximal crescentic metatarsal osteotomy and proximal horizontal "V" osteotomy. On physical examination, the cuneiform is stabilized in a single hand while the first metatarsal is translated superiorly and inferiorly with the other hand. In the presence of mild osteoarthritic modifications, an active individual who understands the possible future need for a fusion might remain a candidate for a corrective osteotomy. Similarly, given the improved medical management of inflammatory arthropathy, an informed patient with well-managed rheumatoid arthritis may also be a candidate for reconstructive hallux valgus surgical procedure quite than fusion. The patient is positioned supine with a small sandbag positioned under the ipsilateral buttock to ensure the foot points up, permitting for simpler osteotomy orientation. Approach We carry out the proximal closing wedge osteotomy with a distal delicate tissue procedure via two incisions.
Syndromes
- Yellow jackets
- Damage to nerves that go to the muscles of the arm, back, and chest wall.
- Blood vessels
- Infection in the brain
- Repeated crying spells
- Abnormal heart rhythms during exercise
- Weakness
- ECG
Generic 150mg rulide amex
The ulnar side of the lunate should be carefully examined for subchondral cysts treatment yellow fever cheap rulide 150mg amex. Mechanical d�bridement of the triangular fibrocartilage has been successful although it can be challenging medications for factor 8 discount rulide 150 mg online, notably in regard to the d�bridement of the ulnar and dorsal features of the triangular fibrocartilage tear medicine you can take while breastfeeding discount rulide 150mg amex. It is mostly thought that an arthroscopically assisted ulnar shortening is indicated if the ulnar-plus variance is lower than 4 mm. Avoid scuffing the articular surfaces while passing the cutting and grasping instruments from the 3-4 portal throughout the radiocarpal joint into the ulnocarpal joint. Occasionally, nonetheless, the devices have to be handed through the 6U portal while the scope is positioned within the 3-4 portal. Injury to the dorsal sensory branch of the ulnar nerve is avoided when establishing the 6U portal through the use of a longitudinal portal incision and blunt dissection to reach the ulnocarpal joint capsule. The presence of popping or clicking is an indication that further d�bridement may be wanted or that some other pathology is inflicting the popping and clicking. With the assistance of a side-firing 70-degree laser tip, the triangular fibrocartilage may be rapidly and exactly d�brided. Arthroscopic ulnar shortening is achieved by putting the scope in the 3-4 portal and introducing the devices via the 4-5 portal. Occasionally the 6U portal can be used, as can the distal distal radioulnar joint portal. It is important to avoid harm to the sigmoid notch, and frequent fluoroscopic monitoring of the amount of bone resected is obligatory. Take care to absolutely supinate and pronate the wrist to adequately d�bride the ulnar head. The 70degree side-firing laser probe simply vaporizes the hyaline cartilage and subchondral bone of the ulnar head. The small joint burr is introduced in through the 4-5 or 6R portal to finish the ulnar shortening. Inappropriate distal placement of the portals can lead to scuffing of the lunate and triquetrum. The dorsal department of the ulnar nerve is in danger during the creation of all ulnar portals. Once the skin is cut, a Hartmann hemostat ought to be used to bluntly dissect via the subcutaneous tissue and penetrate the wrist joint capsule. Small transverse incisions in Langer lines closed with a subcuticular Prolene produce a superior beauty result. The assistant must take the wrist from full supination to full pronation while the operator maintains the arthroscope within the 3-4 portal and the instruments in the ulnar portals. Premature resumption of heavy lifting or repetitive activities will result in ulnocarpal synovitis. Typically patients are capable of return to unrestricted actions in 12 weeks, though they could expertise some discomfort for six to 12 months. We have seen one affected person reconstitute his triangular fibrocartilage and require repeat d�bridement. The surgeon should avoid extreme ulnar d�bridement, which could result in the detachment of the triangular fibrocartilage from the fovea. Long-term results after arthroscopic resection of lesions of the triangular fibrocartilage complex. Clinical outcomes of treatment of triangular fibrocartilage advanced tears by arthroscopic debridement. Relationship between ulnar variance and triangular fibrocartilage advanced thickness. Ulnar variance defines the relationship of the size of the ulna to that of the radius. Ulnar-positive variance can be the end result of a congenital anomaly; traumatic radial shortening from a distal radius, Essex-Lopresti, or Galeazzi fracture; injury to the distal radius physis; or a variant of normal anatomy. The radius articulates with and rotates around the ulnar head through the sigmoid notch. The sigmoid notch has well-defined dorsal, palmar, and distal margins, whereas the proximal margin is indistinct. The interosseous membrane is a fancy construction with a thickened central portion. The diaphysis of the distal half of the ulna is supplied by small segmental branches from the anterior and posterior interosseous arteries. These enter the ulna in 1- to 3-cm intervals from the direction of the interosseous membrane and should be protected in the course of the surgical strategy. The ulnolunate and ulnotriquetral ligaments originate from the ulnar fovea and move palmar to the palmar radioulnar ligament. Deterioration of the ulnocarpal constructions is quite common regardless of ulnar variance. Characterization of the ache Description of the location, duration, and radiation of the ache as properly as any related swelling, burning or tingling sensations, or sounds (clicks, etc. Table 1 Percentage of Force Transmitted Through the Ulna (Nine Arms) Amount removed of the articular disk of the triangular fibrocartilage complex None 1/3 2/3* All* 17. A palmar sag and a supination posture of the wrist might indicate the capsuloligamentous instability that happens in rheumatoid arthritis. Swelling, bruising, perforations of the skin, or apparent dislocations may point out trauma. Splinter hemorrhages beneath the nails and decreased turgor within the volar digital pads suggests vascular insufficiency. Single-finger palpation ought to proceed in a scientific style by isolating anatomic structures. Specific provocative exams should be carried out in an attempt to further outline the injured structure(s). Ulnar compression test: A constructive test is exacerbation of pain, which suggests arthritis or instability; dorsal or palmar subluxation may be famous. These are obtained with the affected person seated and the elbow flexed at 90 degrees and the shoulder kidnapped at 90 levels. Radiographic assessment of ulnar variance has used a impartial rotation radiographic view of the wrist that provides an image of the radioulnar length with the wrist unloaded. Arthroscopy can affirm a analysis instructed by findings from other diagnostic modalities. Bone scan, ultrasonography, and computed tomography serve a very restricted role within the prognosis of ulnar impaction syndrome. Ice and elevation may assist to scale back any swelling associated with overuse or aggravation of a previous damage. Nonsteroidal anti-inflammatory drugs will also cut back swelling and supply some analgesia. Neutral splinting supplies help for the wrist and may assist to stop aggravating maneuvers.
Purchase rulide 150 mg overnight delivery
Return of a muscle action potential requires not only regeneration of the nerve to the level of the top organ but also re-establishment of a physiologic connection between the nerve and the goal tissue medicine x 2016 buy rulide 150mg overnight delivery. Continuity of the nerve also may be assessed symptoms vitamin b12 deficiency order rulide 150 mg, but must be undertaken at about 10 days after the harm to prevent faulty results medicine natural buy discount rulide 150mg line, as a result of the axons distal to an entire transection could proceed to conduct throughout this initial period after harm. Electrodiagnostic testing must be used on this occasion to outline the extent of damage. Longer delays could compromise the efficacy of surgical restore, secondary to end organ degenerative modifications. Focal accidents are normally observed for shorter durations, as a result of the extent of the injured nerve section usually is smaller. Blunt or blast injuries could additionally be observed for up to 6 months given the customarily large segments of injured nerve undergoing repair. If nerve grafts could also be required, the opposite leg is prepared to enable entry to the sural nerve. Rarely, if bilateral sural nerves are to be harvested, the patient initially is placed susceptible. Use of a tourniquet could result in ischemic conduction blocks, which can render intraoperative nerve stimulation ineffective. It generally is preferable to use a tourniquet for only the first 20 minutes of surgical procedure, to facilitate preliminary dissection. The use of an operating microscope and nice gentle tissue sets or microinstrumentation is important for nerve dealing with and restore. Approach Surgical publicity ought to present enough access to the part of broken nerve as nicely as proximal and distal to this site. Mobilization ought to be minimized to stop additional vascular insult to the nerve. The median nerve at the wrist developed painful scarring after carpal tunnel launch. External neurolysis has been performed by excision of all scar tissue and thickened epineurium. Appearance after inner neurolysis-the constricting epineurium and scar between fascicles has been excised. The phase of scarred epineurium is excised, and all scar tissue between fascicles also is excised. This process is carried out in instances of incomplete practical loss distal to the location of damage. Some lack of intact axons can be anticipated as a result of the dissection, so the affected person should be advised that further lack of operate could probably be potential with this process. The posterior interosseous nerve demonstrates a neuroma in continuity (white arrow). Internal neurolysis has been carried out, isolating intact peripheral fascicles with a central neuroma (white arrow). Nonconducting fascicular segments are excised and either repaired by end-to-end group fascicular restore (E) or by interposing nerve grafts (F). Cable grafting is the more widespread technique, utilizing donor nerve from either the sural or antebrachial cutaneous nerve. The internal arrangement of the fascicles is famous, and a fast sketch of the fascicular association is made to enable alignment of the nerve ends. The hole between nerve ends is measured, and the length of graft wanted is calculated. Length gap 15% estimated number of grafts Grafts are hooked up to a bunch of fascicles using two sutures of 9-0 or 10-0 nylon, one hundred eighty degrees from each other. Each graft is sutured to the proximal and distal stumps before transferring on to the subsequent graft, thus allowing for more accurate fascicular matching. The repair could additionally be reinforced with fibrin glue Handling of the grafts should be minimized. The proximal and distal portions of the nerve flanking the lesion ought to be mobilized to stop undue rigidity on the restore. The lesion is sharply excised using a recent, sharp blade against a block (usually a moistened tongue depressor). Epineurial Repair If the extent of the lesion is short, then direct end-to-end epineurial restore with out rigidity typically is possible. Yellow rubber slings have been positioned around the nerve at each incision for identification and delicate traction to facilitate dissection. Multiple segments of the sural nerve have been aligned and inserted within the nerve gap and fixed with group fascicular sutures. Focal accidents may be noticed for 2 to three months, whereas lengthy lesions may be noticed for as much as 5 months. A mixture of medical and electrodiagnostic testing should be used to consider an damage. Avoid lengthy durations of observation in the absence of progressive signs of recovery as irreversible end organ injury could result. Internal neurolysis or resection of any lesion in continuity could also be associated to a decrease in preoperative perform as some intact axons may be transected. Complete resection with direct repair or graft repair the result of direct repairs appears to be superior to those requiring the usage of a graft; nevertheless, injuries requiring a nerve graft usually are extra substantial and require regeneration alongside a larger distance. In common, radial nerve repairs are more profitable than median nerve repairs, and each are better than ulnar nerve repairs. Tubular versus conventional restore of median and ulnar nerves in the human forearm: Early outcomes from a prospective, randomized, medical examine. Intraoperative nerve recordings as a helpful aid in the management of neuroma-in-continuity. Palsy of the median nerve can lead to motor or sensory deficits, or both, inside the distribution of this nerve. Over a interval of months to years, patients can progress to decreased median nerve function in addition to sensory changes in the dermatome of this nerve. Acute accidents to the median nerve on the wrist or elbow have a traumatic onset followed by sensory or motor modifications, or both. The median nerve travels down the forearm between the flexor digitorum superficialis and profundus muscular tissues to enter the carpal tunnel. The palmar cutaneous branch arises from the median nerve 5 cm proximal to the wrist joint, crosses the wrist volar to the transverse carpal ligament, and supplies sensibility to the thenar eminence. Just proximal to the wrist, the median nerve turns into superficial and travels throughout the carpal tunnel. The recurrent motor department originates from the central or radial portion of the median nerve during its passage via the carpal tunnel.
Order rulide 150 mg otc
Last week she had a low-grade fever and generalized malaise medicine man dr dre safe rulide 150mg, which has since resolved symptoms 89 nissan pickup pcv valve bad cheap rulide 150mg without prescription. She has had 4 new sexual partners in the final 12 months and makes use of oral contraceptives symptoms low blood pressure buy rulide 150mg free shipping. She is sexually energetic in a monogamous relationship with a male companion of 5 years and he or she uses a contraceptive ring (NuvaRing). Women identified with this condition ought to be recommended concerning which of the next Risk factors for creating this condition embrace the entire following besides: a. She recently tried an over-the-counter antifungal remedy A solutions Vignette 1 Question four Answer C: Because of the excessive rate of concomitant Trichomonas infections in sexual companions, all partners should be handled to prevent reinfection. This is most likely going due to the high efficacy of nitroimidazole medication, with a 90% to 95% cure rate. Vignette 1 Question 5 Answer B: Metronidazole 500 mg orally twice a day for 7 days is recommended for circumstances of metronidazole single-dose remedy failure. Treatment with tinidazole 2 g orally day by day for 5 days is recommended after therapy failure with both the single-dose and the multidose metronidazole regimens. Consultation with infectious illness specialist is really helpful just for refractory cases after a quantity of treatment failures. Nitroimidazoles are the only class of drugs helpful for the therapy of Trichomonas infections. Pap smears should begin at 21 years of age regardless of age at first intercourse. A diagnosis of chlamydial infection or gonorrhea ought to be made prior to remedy. Vaginal cultures may be helpful if yeast or trichomoniasis is suspected and microscopy is normal. The sensitivity of Gram stain to the analysis of chlamydial an infection or gonorrhea is low. In addition, the patient Vignette 1 Question 1 Answer D: the symptoms and findings are most according to Trichomonas. Symptomatic patients report a frothy vaginal discharge that might be yellow, grey, or green. The classical cervical findings include erythematous, punctate epithelial papillae, or "strawberry" appearance. Symptoms embrace vaginal burning, pruritus, and increased thick, white, curdy vaginal discharge. Multinucleated giant cells can be seen on Tzanck smear preparation of herpetic lesions. Vignette 1 Question 2 Answer C: Trichomoniasis is attributable to Trichomonas vaginalis. Vignette 1 Question three Answer A: A single-dose routine with metronidazole or tinidazole is the mainstay therapy of trichomoniasis. An different multidose routine is metronidazole 500 mg orally twice every day for 7 days. Clindamycin can be used as an alternative routine for the treatment of bacterial vaginosis. Metronidazole gel is considerable much less efficacious for the therapy of trichomoniasis. Vignette 3 Question three Answer C: For main genital herpes infections, acyclovir 200 mg orally 5 occasions day by day for 7 to 10 days is beneficial to reduce the length of infection and the size of time a affected person has viral shedding. Other choices embrace a 7 to 10 day oral remedy with acyclovir 400 mg 3 times per day, famciclovir 250 mg three times per day, or valacyclovir 1 g twice per day. Extended regimens of doxycycline can be used to deal with lymphogranuloma venereum attributable to C. Vignette 3 Question 4 Answer D: Viral shedding can occur each with and with out genital herpes symptoms. Subclinical viral shedding appears to be highest within the first 6 months following acquisition and is extra widespread instantly before and after a clinical outbreak. Both symptomatic and asymptomatic viral shedding can happen in genital areas not covered or protected by a condom. Recurrent outbreaks may be lowered via using daily suppressive antiviral medication. Cesarean supply is beneficial only for those pregnant sufferers with energetic genital lesions or prodromal symptoms. Patients normally complain of an elevated vaginal discharge that often has a malodorous fishy amine odor. Alternatives embody clindamycin 300 mg twice a day for 7 days or topical formulations of these antibiotics. Azithromycin 1 g orally as quickly as is also the right treatment option for chlamydial an infection. Unless chlamydial co-infection has been dominated out, sufferers identified with gonorrhea must be empirically handled for chlamydial an infection with ceftriaxone and azithromycin. Doxycycline 100 mg orally twice day by day for 7 days is the right therapy for chlamydial an infection. Because of accelerating resistance, fluoroquinolones are now not recommended within the United States for the treatment of gonorrhea. Vignette three Question 1 Answer B: Genital herpes classically presents with painful clusters of small vesicles and ulcers. Moreover, primary infections normally start with flulike symptoms including malaise, myalgias, nausea, diarrhea, and fever. She is sexually lively and uses Depo-Provera A solutions examinations, extended rupture of membranes, inner fetal monitoring, low socioeconomic standing, guide removing of the placenta, and extended labor. However, medical manifestations of ectopic pregnancies typically seem 6 to 7 weeks after the last regular menstrual interval. Women also usually have vaginal bleeding, pain, and signs of early being pregnant. The prognosis is basically made clinically with findings of fever and uterine tenderness in a postpartum girl. Pyelonephritis should be suspected in a affected person with fever, flank pain, and costovertebral angle tenderness. The hematuria on this affected person is probably going because of contamination from the lochia postpartum. Chorioamnionitis or intraamniotic an infection is a maternal febrile morbidity exclusive to the intrapartum period. Septic pelvic thrombophlebitis is usually a prognosis of exclusion and ought to be considered within the setting of persistent unexplained fever in the postpartum interval. This affected person has a traditional showing incision making wound cellulitis most unlikely. Vignette 1 Question 2 Answer E: Postpartum endomyometritis is typically a polymicrobial an infection involving both aerobes and anaerobes from the genital tract. Treatment course continues till scientific improvement and afebrile status for twenty-four to 48 hours.
References
- Dempsey D, Tutka P, Jacob P III, et al. Nicotine metabolite ratio as an index of cytochrome P450 2A6 metabolic activity. Clin Pharmacol Ther 2004; 76(1):64-72.
- Naroda T, Yamanaka M, Matsushita K, et al: Clinical studies for venogenic impotence with color Doppler ultrasonographyoevaluation of resistance index of the cavernous artery, Nippon Hinyokika Gakkai Zasshi 87:1231n1235, 1996.
- Marshall LF, Camp PE, Bowers SA. Dimethyl sulfoxide for the treatment of intracranial hypertension: A preliminary trial. Neurosurgery. June 1984;14(6):659-663.
- Moriarty AS, Gilbody S, McMillan D, et al: Screening and case finding for major depressive disorder using the Patient Health Questionnaire (PHQ-9): a meta-analysis, Gen Hosp Psychiatry 37:567n576, 2015.