
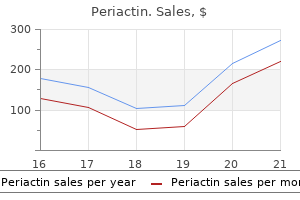
Periactin
Tammy Bryant, RN, BSN
- Program Director
- Southwest Georgia Technical College
- Thomasville, Georgia
Periactin dosages: 4 mg
Periactin packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Generic periactin 4 mg mastercard
Septic shock Refractory septic shock a Fluid resuscitation is taken into account adequate when the pulmonary artery wedge pressure is 12 mmHg or the central venous strain is eight mmHg allergy symptoms skin periactin 4 mg for sale. Fever or hypothermia allergy kid recipes cheap 4mg periactin amex, leukocytosis or leukopenia allergy symptoms to wheat buy periactin 4 mg low cost, tachypnea, and tachycardia are cardinal signs of the systemic response. In general, when an infectious etiology is confirmed or strongly suspected and the response ends in hypofunction of uninfected organs, the time period sepsis (or severe sepsis) must be used. In fact, blood cultures yield bacteria or fungi in solely ~20�40% of circumstances of extreme sepsis and 40�70% of cases of septic shock. Microbiologic outcomes were optimistic in 70% of people considered infected; of the isolates, 62% have been gram-negative micro organism (Pseudomonas species and Escherichia coli have been most common), 47% were grampositive micro organism (Staphylococcus aureus was most common), and 19% had been fungi (Candida species). This distribution is much like that reported a decade earlier from eight educational centers within the United States (Table 325-2). The incidence of severe sepsis and septic shock has increased over the past 30 years, and the annual number of cases is now >750,000 (~3 per 1000 population). Approximately two-thirds of the instances happen in patients with important underlying sickness. Sepsis-related incidence and mortality rates improve with age and preexisting comorbidity. The widespread use of immunosuppressive drugs, indwelling catheters, and mechanical gadgets has additionally played a role. Invasive bacterial infections are outstanding causes of demise around the world, particularly among younger youngsters. In sub-Saharan Africa, for instance, cautious screening for constructive blood cultures discovered that community-acquired bacteremia accounted for no much less than one-fourth of deaths of kids >1 year of age. Nontyphoidal Salmonella species, Streptococcus pneumoniae, Haemophilus influenzae, and E. To survive throughout the human physique, these microbes typically exploit acquired deficiencies in host defenses, indwelling catheters or other foreign matter, or obstructed fluid drainage conduits. Microbial pathogens, in contrast, can circumvent innate defenses because they (1) lack molecules that may be acknowledged by host receptors (see below) or (2) elaborate toxins or other virulence factors. In both circumstances, the body can mount a vigorous inflammatory response that results in sepsis or septic shock but fails to kill the invaders. The septic response can also be induced by microbial exotoxins that act as superantigens. Host Mechanisms for Sensing Microbes Animals have exquisitely delicate mechanisms for recognizing and responding to sure extremely conserved microbial molecules. Most of the commensal cardio and facultatively anaerobic gram-negative micro organism that set off extreme sepsis and shock (including E. When these bacteria enter the physique, they might initially induce relatively little inflammation. Local and Systemic Host Responses to Invading Microbes Recognition of microbial molecules by tissue phagocytes triggers the production and/or launch of numerous host molecules (cytokines, chemokines, prostanoids, leukotrienes, and others) that improve blood move to the infected tissue (rubor), improve the permeability of native blood vessels (tumor), recruit neutrophils and different cells to the positioning of infection (calor), and elicit pain (dolor). Systemic responses are activated by neural and/or humoral communication with the hypothalamus and brainstem; these responses enhance local defenses by increasing blood flow to the infected area, augmenting the number of circulating neutrophils, and elevating blood ranges of numerous molecules (such as the microbial recognition proteins mentioned above) which have antiinfective capabilities. The nonlinearity and multiplicity of these interactions have made it tough to interpret the roles performed by individual mediators in each tissues and blood. Clotting can also be favored by impaired function of the protein C�protein S inhibitory pathway and depletion of antithrombin and proteins C and S, whereas fibrinolysis is reduced by increases in plasma ranges of plasminogen activator inhibitor 1. Thus, there could also be a hanging propensity toward intravascular fibrin deposition, thrombosis, and bleeding; this propensity has been most obvious in sufferers with intravascular endothelial infections such as meningococcemia (Chap. Evidence points to tissue factor�expressing microparticles derived from leukocytes as a possible set off for intravascular coagulation. Local control mechanisms Host recognition of invading microbes inside subepithelial tissues typically ignites immune responses that quickly kill the invaders and then subside to enable tissue recovery. The forces that put out the hearth and clean up the battleground embody molecules that neutralize or inactivate microbial signals. Systemic control mechanisms the signaling apparatus that hyperlinks microbial recognition to mobile responses in tissues is less active in the blood. Glucocorticoids inhibit cytokine synthesis by monocytes in vitro; the increase in blood cortisol ranges that happens early within the systemic response presumably performs a similarly inhibitory function. Other acute-phase proteins are protease inhibitors or antioxidants; these may neutralize doubtlessly harmful molecules released from neutrophils and different inflammatory cells. It could thus be stated that each native and systemic responses to infectious agents benefit the host in necessary methods. Most of those responses and the molecules liable for them have been highly conserved throughout animal evolution and subsequently may be adaptive. Although high concentrations of both pro- and anti-inflammatory molecules are found, the net mediator steadiness within the plasma of those extremely sick sufferers seems to be anti-inflammatory. In addition, regulated cell-adhesion molecules promote the adherence of neutrophils to endothelial cells. Tissue oxygenation may lower because the number of useful capillaries is reduced by luminal obstruction due to swollen endothelial cells, decreased deformability of circulating erythrocytes, leukocyteplatelet-fibrin thrombi, or compression by edema fluid. On the other hand, research using orthogonal polarization spectral imaging of the microcirculation within the tongue discovered that sepsis-associated derangements in capillary circulate could possibly be reversed by making use of acetylcholine to the floor of the tongue or by giving nitroprusside intravenously; these observations suggest a neuroendocrine basis for the loss of capillary filling. The local accumulation of lactic acid, a consequence of elevated glycolysis, may decrease extracellular pH and contribute to the slowdown in cellular metabolism that happens within affected tissues. Before this vasodilatory phase, many patients experience a interval during which oxygen delivery to tissues is compromised by myocardial despair, hypovolemia, and different factors. During this "hypodynamic" interval, the blood lactate focus is elevated and central venous oxygen saturation is low. Fluid administration is normally followed by the hyperdynamic vasodilatory section, throughout which cardiac output is regular (or even high) and oxygen consumption declines despite sufficient oxygen delivery. The blood lactate degree may be normal or elevated, and normalization of central venous oxygen saturation might mirror improved oxygen delivery, decreased oxygen uptake by tissues, or left-to-right shunting. Prominent hypotensive molecules include nitric oxide, -endorphin, bradykinin, platelet-activating issue, and prostacyclin. In most sufferers infected with different gram-negative micro organism, in contrast, circulating bacteria or bacterial molecules could replicate uncontrolled infection at a neighborhood tissue website and have little or no direct influence on distant organs; in these patients, inflammatory mediators or neural alerts arising from the local web site appear to be the key triggers for extreme sepsis and septic shock. In a big sequence of patients with optimistic blood cultures, the chance of developing extreme sepsis was strongly related to the location of major an infection: bacteremia arising from a pulmonary or stomach source was eightfold extra more probably to be associated with extreme sepsis than was bacteremic urinary tract an infection, even after the investigators controlled for age, the kind of bacteria isolated from the blood, and different factors. A third pathogenesis may be represented by extreme sepsis because of superantigen-producing S. Genetic components are in all probability important as nicely, but despite a lot study very few allelic polymorphisms have been related to sepsis severity in more than one or two analyses. The price at which extreme sepsis develops might differ from affected person to patient, and there are putting particular person variations in presentation.
4 mg periactin overnight delivery
Survival probabilities in public websites exceed those within the residence surroundings allergy treatment jobs in quad cities discount 4 mg periactin fast delivery, where the vast majority of cardiac arrests happen allergy diet order 4mg periactin overnight delivery. The probability of progression to biologic dying is a function of the mechanism of cardiac arrest and the length of the delay before interventions allergy nebraska generic periactin 4mg online. However, there are few survivors among patients who had no life assist actions for the first 8 min after onset. Anoxic encephalopathy and infections subsequent to prolonged respirator dependence account for 60% of the deaths. Recurrent arrhythmias are the least common cause of death, accounting for much less than 10% of in-hospital deaths. Primary cardiac arrests are those who happen within the absence of hemodynamic instability, and secondary cardiac arrests are those that occur in sufferers in whom irregular hemodynamics dominate the scientific image earlier than cardiac arrest. In contrast, as many as 70% of sufferers with secondary cardiac arrest succumb instantly or throughout the identical hospitalization. The initial response, together with confirmation of loss of circulation, followed by basic life support and public access defibrillation, can be carried out by physicians, nurses, paramedical personnel, and educated laypersons. As soon as a cardiac arrest is suspected, confirmed, and even thought-about to be impending, calling an emergency rescue system. In truth, continued gasping is taken into account a great prognostic signal for profitable consequence. It can also be necessary to observe for severe stridor with a persistent pulse as a clue to aspiration of a overseas body or food. Therefore, it is strongly recommended to use precordial thumps as a life help method only when monitoring and defibrillation can be found. The head is tilted back and the chin lifted so that the oropharynx can be explored to clear the airway. Closed chest cardiac compression maintains a pump function by sequential filling and emptying of the chambers, with competent valves maintaining forward course of move. The palm of 1 hand is positioned over the decrease sternum, with the heel of the opposite resting on the dorsum of the lower hand. The sternum is depressed, with the arms remaining straight, at a price of a hundred per minute. Sufficient force is utilized to depress the sternum 4�5 cm, and relaxation is abrupt. This advance has inserted one other stage of response into the cardiac arrest paradigm. Chest compressions should be carried out while the defibrillator is being charged. Multiple shocks given in sequence are 1769 not really helpful, in order to minimize interruptions of chest compressions. The actions carried out to obtain these objectives include (1) defibrillation/cardioversion and/or pacing, (2) intubation with an endotracheal tube, and (3) insertion of an intravenous line. If the patient is less than fully conscious upon reversion or if two or three attempts fail, immediate intubation, ventilation, and arterial blood fuel evaluation ought to be carried out. Quantitative waveform capnography is now really helpful for affirmation and monitoring of endotracheal tube placement. The algorithm of ventricular fibrillation or pulseless ventricular tachycardia begins with and preliminary defibrillate on attempt. After three such sequences, epinephrine and then antiarrhythmic drugs are added to the protocol. The algorithms for bradyarrhythmia/asystole (left) or pulseless electrical exercise (right) are dominated first by continued life help and a seek for reversible causes. After initial unsuccessful defibrillation attempts or with persistent/ recurrent electrical instability, antiarrhythmic remedy should be instituted. Intravenous amiodarone has emerged as the initial therapy of choice (150 mg over 10 min, adopted by 1 mg/min for as much as 6 h and 0. Cardiac arrest as a end result of bradyarrhythmias or asystole (B/A cardiac arrest) is managed differently. External pacing gadgets are used to attempt to establish an everyday rhythm when atropine fails for a bradyarrhythmia, but chronotropic agents given intravenously are actually recognized as an equally efficient alternative. For acute airway obstruction, immediate removal of foreign bodies by the Heimlich maneuver or, in hospitalized sufferers, by intubation and suctioning of obstructing secretions within the airway is often profitable. The prognosis is usually very poor in other causes of this type of cardiac arrest, corresponding to end-stage cardiac or noncardiac diseases. This recently developed clinical classification emerged from the group of the elements of harm following cardiac arrest into a multidisciplinary continuum. The 4 elements of post-cardiac arrest syndrome include brain damage, myocardial dysfunction, systemic ischemia/reperfusion responses, and control of persistent precipitating elements. The therapeutic aim is to preserve a stable electrical, hemodynamic, and central nervous system standing. The most pressing is the presence of anoxic encephalopathy, which is a robust predictor of in-hospital demise and postarrest disability. Core body temperature is decreased to 32�34�C, by a number of out there methods (external and/or inside [core]), as soon as practical after resuscitation and maintained for a minimum of 12�24 h. By decreasing metabolic demands and cerebral edema, this intervention improves likelihood of survival with higher neurologic outcome. In the in-hospital setting, respirator help is normally not necessary or is required for only a quick time, and hemodynamics stabilize promptly after defibrillation or cardioversion. Patients with end-stage most cancers, renal failure, acute central nervous system disease, and uncontrolled infections, as a bunch, have a survival rate of <10% after in-hospital cardiac arrest. Some major exceptions are patients with transient airway obstruction, electrolyte disturbances, proarrhythmic results of medicine, and severe metabolic abnormalities, most of whom might have a great likelihood of survival if they can be resuscitated promptly and stabilized while the transient abnormalities are being corrected. Survivors of cardiac arrest as a outcome of different categories of illness, such as the hypertrophic or dilated cardiomyopathies and the various rare inherited problems. Total mortality advantages in the range of a 20�35% discount over 2�5 years have been observed in a collection of medical trials. Decision making for main prevention in issues other than coronary artery disease and dilated cardiomyopathy is usually pushed by observational information and judgment primarily based on clinical observations. Akinetic mutism refers to a partially or absolutely awake state in which the patient is prepared to form impressions and suppose, as demonstrated by later recounting of events, but stays virtually immobile and mute. The situation results from injury within the regions of the medial thalamic nuclei or the frontal lobes (particularly lesions situated deeply or on the orbitofrontal surfaces) or from excessive hydrocephalus. The term abulia describes a milder form of akinetic mutism characterised by mental and physical slowness and diminished capacity to provoke exercise. It is also usually the result of harm to the frontal lobes and its connections (Chap. Catatonia is a curious hypomobile and mute syndrome that occurs as a half of a serious psychosis, normally schizophrenia or major despair. Catatonic patients make few voluntary or responsive actions, although they blink, swallow, and will not appear distressed. There are nonetheless signs that the affected person is responsive, though it could take ingenuity on the a part of the examiner to show them.
Diseases
- Scalp defects postaxial polydactyly
- Quadrantanopia
- Rectophobia
- Behrens Baumann Dust syndrome
- Rambam Hasharon syndrome
- Porphyria, congenital erythropoietic
Buy 4mg periactin free shipping
Genetic defects as in hereditary pancreatitis and cystic fibrosis mutations can end result in recurrent pancreatitis allergy treatment while pregnant buy periactin 4mg online. Other ailments of the biliary tree and pancreatic ducts that may cause acute pancreatitis embody choledochocele; ampullary tumors; pancreas divisum; and pancreatic duct stones allergy with fever periactin 4mg on line, stricture allergy medicine active ingredients cheap 4 mg periactin with mastercard, and tumor. Approximately 2�4% of sufferers with pancreatic carcinoma present with acute pancreatitis. A recent randomized trial reported advantages 2098 trimethoprim-sulfamethoxazole, and protease inhibitors. The events that provoke and then perpetuate the inflammatory process within the pancreas have gotten more clearly understood. Thus, the situation is defined by the presence of histologic abnormalities, including continual irritation, fibrosis, and progressive destruction of each exocrine and finally endocrine tissue (atrophy). A variety of etiologies have been associated with persistent pancreatitis resulting within the cardinal manifestations of the disease corresponding to stomach pain, steatorrhea, weight loss, and diabetes mellitus (Table 371-5). Although alcohol has been believed to be the primary reason for chronic pancreatitis, other components contribute to the disease because not all heavy consumers of alcohol develop pancreatic disease. Smoking is an impartial, dose-dependent risk issue for persistent pancreatitis and recurrent acute pancreatitis. As many as 25% of adults within the United States with chronic pancreatitis have the idiopathic type. Recent investigations have indicated that as much as 15% of sufferers with idiopathic pancreatitis could have pancreatitis due to genetic defects (Table 371-5). Whitcomb and associates studied a quantity of large households with hereditary chronic pancreatitis and have been in a position to determine a genetic defect that impacts the gene encoding for trypsinogen. The defect prevents the destruction of prematurely activated trypsin and allows it to be immune to the intracellular protecting effect of trypsin inhibitor. It is hypothesized that this continuous activation of digestive enzymes throughout the gland results in acute harm and, lastly, persistent pancreatitis. Attempts to elucidate the relationship between the genotype and pancreatic manifestations have been hampered by the number of mutations. In addition, the therapeutic and prognostic implication of these findings with respect to managing pancreatitis stays to be decided. A research evaluated 39 sufferers with idiopathic persistent pancreatitis to assess the danger associated with these mutations. Table 371-5 lists recognized causes of persistent pancreatitis and pancreatic exocrine insufficiency. The attribute pancreatic histopathologic findings include lymphoplasmacytic infiltrate, storiform fibrosis, and plentiful IgG4 cells. Mild signs, often stomach pain, and recurrent acute pancreatitis are uncommon. Elevated serum ranges of IgG4 present a marker for the illness, notably in Western populations. Characteristic histologic findings include intensive lymphoplasmacytic infiltrates with dense fibrosis around pancreatic ducts, in addition to a lymphoplas- 2099 macytic infiltration, resulting in an obliterative phlebitis. Patients might respond dramatically to glucocorticoid therapy inside a 2- to 4-week interval. Prednisone is usually administered at an initial dose of forty mg/d for 4 weeks adopted by a taper of the daily dosage by 5 mg/wk primarily based on monitoring of scientific parameters. A poor response to glucocorticoids over a 2- to 4-week interval should increase suspicion of pancreatic cancer or other forms of chronic pancreatitis. A small number of patients responded favorably to 6-mercaptapurine, rituximab, cyclosporine, and cyclophosphamide. Relapse is common in type 1 sufferers, particularly these with biliary tract strictures. Patients with refractory signs and strictures typically require immunomodulator therapy as famous above. Clinical Features of Chronic Pancreatitis Patients with continual pancreatitis search medical attention predominantly because of two signs: belly ache or maldigestion and weight reduction. Eating might exacerbate the pain, resulting in a concern of eating with consequent weight reduction. Maldigestion is manifested as persistent diarrhea, steatorrhea, weight loss, and fatigue. Patients with persistent stomach pain may or could not progress to maldigestion, and ~20% of sufferers will current with signs of maldigestion without a historical past of abdominal pain. Patients with continual pancreatitis have important morbidity and mortality and use appreciable amounts of societal resources. Despite steatorrhea, clinically apparent deficiencies of fat-soluble vitamins are surprisingly uncommon. Many patients have impaired glucose tolerance with elevated fasting blood glucose ranges. The fecal elastase-1 and small-bowel biopsy are useful in the evaluation of sufferers with suspected pancreatic steatorrhea. The fecal elastase degree might be abnormal and small-bowel histology shall be regular in such sufferers. A decrease of fecal elastase degree to <100 g per gram of stool strongly suggests extreme pancreatic exocrine insufficiency. The radiographic evaluation of a affected person with suspected persistent pancreatitis often proceeds from a noninvasive to more invasive method. The secretin test becomes abnormal when 60% of the pancreatic exocrine function has been misplaced. Diffuse calcifications famous on plain movie of the stomach often point out important injury to the pancreas and are pathognomic for chronic pancreatitis. Although alcohol is by far the commonest explanation for pancreatic calcification, such calcification may be noted in hereditary pancreatitis, posttraumatic pancreatitis, hypercalcemic pancreatitis, idiopathic chronic pancreatitis, and tropical pancreatitis. Complications of Chronic Pancreatitis the issues of chronic pancreatitis are protean and are listed in Table 371-7. Although most patients have impaired glucose tolerance, diabetic ketoacidosis and diabetic coma are uncommon. Gastrointestinal bleeding might happen from peptic ulceration, gastritis, a pseudocyst eroding into the duodenum, arterial bleeding into the pancreatic duct (hemosuccus pancreaticus), or ruptured varices secondary to splenic vein thrombosis because of persistent inflammation of the tail of the pancreas. Jaundice, cholestasis, and biliary cirrhosis could occur from the persistent inflammatory response across the intrapancreatic portion of the frequent bile duct. Patients with hereditary pancreatitis are at a 10-fold larger threat for pancreatic most cancers. Note the markedly dilated pancreatic duct seen in this part through the physique and tail (open arrows). Enzyme therapy often brings diarrhea beneath control and restores absorption of fat to a suitable degree and impacts weight achieve. In treating steatorrhea, it is very important use a potent pancreatic formulation that will ship sufficient lipase into the duodenum to right maldigestion and reduce steatorrhea.
Buy periactin 4mg visa
When present allergy symptoms journal generic periactin 4mg, microvascular dysfunction is related to a larger infarct size allergy symptoms 4dp5dt buy periactin 4 mg lowest price, coronary heart failure allergy bomb periactin 4mg with amex, malignant ventricular arrhythmias, and demise. The "offender" ruptured plaque and residual thrombus at the moment are obvious in the vessel. The ultimate outcome reveals no residual stenosis in either the ramus or second obtuse marginal vessels. It happens most commonly throughout the first month, however not often can occur as late as 1 year (0. He received dual antiplatelet remedy with aspirin and clopidogrel for 1 yr and then discontinued clopidogrel per protocol. A magnified view of the vessel reveals thrombus across the stent strut and neointima formation (arrow) (right). Follow-up echocardiograms to assess for gadget migration or erosion, residual shunting, thrombus, or pericardial effusion are beneficial at 1 day, 1 month, 6 months, 1 12 months, and periodically thereafter. It usually is related to further cardiovascular disease threat factors, and the danger of cardiovascular disease increases with the entire burden of threat elements. Although antihypertensive remedy reduces the risks of cardiovascular and renal disease, giant segments of the hypertensive population are both untreated or inadequately handled. Hypertension is present in all populations except for a small number of people dwelling in developing countries. In industrialized societies, blood strain increases steadily through the first 20 years of life. In children and adolescents, blood pressure is associated with progress and maturation. In the United States, common systolic blood pressure is greater for men than for women during early maturity, though among older individuals the age-related price of rise is steeper for women. Consequently, amongst people age 60 and older, systolic blood pressures of women are higher than those of men. Among adults, diastolic blood strain additionally increases progressively with age until ~55 years, after which it tends to lower. The chance of hypertension increases with age, and among people age 60, the prevalence is 65. Recent proof suggests that the prevalence of hypertension in the United States could also be increasing, probably as a consequence of accelerating obesity. Both environmental and genetic factors might contribute to regional and racial variations in hypertension prevalence. The urine sodium-to-potassium ratio (an index of both sodium and potassium intakes) is a stronger correlate of blood stress than is either sodium or potassium alone. Alcohol consumption, psychosocial stress, and low levels of physical activity additionally could contribute to hypertension. Family research controlling for a standard setting point out that blood strain heritabilities are in the vary 15�35%. In twin studies, heritability estimates of blood pressure are ~60% for males and 30�40% for females. However, to date, solely a fraction of high heritability estimates are accounted for by particular genetic determinants. Further, different subsets of genes could result in totally different phenotypes associated with hypertension. Several strategies are getting used in the seek for specific hypertension-related genes. Animal models (including selectively bred rats and congenic rat strains) present a robust approach for evaluating genetic loci and genes related to hypertension. The alpha-adducin gene is thought to be associated with increased renal tubular absorption of sodium, and variants of this gene may be related to hypertension and salt sensitivity of blood stress. Genomewide affiliation research contain quickly scanning markers across the whole genome to identify loci (not specific genes) associated with an observable trait. This strategy has been facilitated by the availability of dense genotyping chips and the International HapMap. Family studies and variations in candidate genes associated with renal harm recommend that genetic components additionally may contribute to hypertensive nephropathy. Peripheral resistance is decided by practical and anatomic modifications in small arteries (lumen diameter 100�400 m) and arterioles. When NaCl intake exceeds the capability of the kidney to excrete sodium, vascular volume could initially broaden and cardiac output may improve. However, many vascular beds have the capability to autoregulate blood circulate, and if fixed blood flow is to be maintained within the face of elevated arterial strain, resistance within that bed should improve, since Blood move = strain throughout the vascular mattress vascular resistance the preliminary elevation of blood stress in response to vascular volume growth may be associated to a rise of cardiac output; nevertheless, over time, peripheral resistance increases and cardiac output reverts toward regular. What is evident is that salt can activate numerous neural, endocrine/paracrine, and vascular mechanisms, all of which have the potential to improve arterial strain. In individuals with an impaired capability to excrete sodium, larger increases in arterial stress are required to obtain natriuresis and sodium stability. NaCl-dependent hypertension could additionally be a consequence of a decreased capability of the kidney to excrete sodium, due both to intrinsic renal disease or to elevated production of a salt-retaining hormone (mineralocorticoid) resulting in elevated renal tubular reabsorption of sodium. Renal tubular sodium reabsorption also could additionally be augmented by elevated neural activity to the kidney. In every of those situations, a better arterial strain may be required to obtain sodium steadiness. In ~80% of these sufferers, vascular quantity and hypertension can be controlled with enough dialysis; within the other 20%, the mechanism of hypertension is said to increased activity of the reninangiotensin system and is prone to be conscious of pharmacologic blockade of renin-angiotensin. Norepinephrine, epinephrine, and dopamine all play important roles in tonic and phasic cardiovascular regulation. In addition to receptor affinity and density, physiologic responsiveness to catecholamines may be altered by the effectivity of receptor-effector coupling at a web site "distal" to receptor binding. Based on their physiology and pharmacology, adrenergic receptors have been divided into two principal varieties: and. Receptors are occupied and activated extra avidly by norepinephrine than by epinephrine, and the reverse is true for receptors. In the kidney, activation of 1-adrenergic receptors will increase renal tubular reabsorption of sodium. For example, orthostatic hypotension incessantly is noticed in patients with pheochromocytoma, probably as a result of the shortage of norepinephrine-induced vasoconstriction with assumption of the upright posture. Conversely, with continual discount of neurotransmitter substances, adrenoreceptors could improve in quantity or be upregulated, leading to increased responsiveness to the neurotransmitter. Chronic administration of agents that block adrenergic receptors may end in upregulation, and abrupt withdrawal of these brokers might pro- 1613 duce a condition of temporary hypersensitivity to sympathetic stimuli. One arterial baroreflex is mediated by stretch-sensitive sensory nerve endings in the carotid sinuses and the aortic arch. Patients with autonomic neuropathy and impaired baroreflex operate might have extremely labile blood pressures with difficult-to-control episodic blood pressure spikes associated with tachycardia. In both normal-weight and overweight people, hypertension often is associated with increased sympathetic outflow. Sympathetic outflow is elevated in obesity-related hypertension and in hypertension associated with obstructive sleep apnea. Baroreceptor activation through electrical stimulation of carotid sinus afferent nerves lowers blood pressure in patients with "resistant" hypertension.
Discount periactin 4 mg line
Colon resection allergy medicine safe during pregnancy cheap 4 mg periactin otc, normally allergy symptoms lilies purchase periactin 4mg on-line, is reserved for sufferers with constipation and outlet obstruction allergy symptoms 4dp3dt cheap periactin 4 mg on line. Transabdominal procedures can be carried out successfully with laparoscopic and, more lately, robotic methods with out increased incidence of recurrence. The objective of the transabdominal approach is to restore normal anatomy by removing redundant bowel and reattaching the supportive tissue of the rectum to the presacral fascia. If complete colonic inertia is present, as defined by a history of constipation and a optimistic sitzmark examine, a subtotal colectomy with an ileosigmoid or rectal anastomosis could additionally be required at the time of rectopexy. Previously, the presence of inner rectal prolapse recognized on imaging studies has been considered a nonsurgical disorder and biofeedback was recommended. However, solely one-third of sufferers will have profitable resolution of symptoms from biofeedback. An opening within the peritoneum is created on the left side of the rectosigmoid junction, and this opening continues down anterior on the rectum into the pouch of Douglas. Mesh is secured to the anterior and lateral portion of the rectum, the vaginal fornix, rectal prolapse the medical approach to the management of rectal prolapse is proscribed and contains stool-bulking brokers or fiber supplementation to ease the method of evacuation. Transabdominal approaches have been associated with decrease recurrence charges, however some patients with significant comorbidities are higher served by a transperineal approach. In both procedures, recurrence at 1 yr was low (<10%) and signs improved in additional than three-fourths of sufferers. One-half of sufferers with fecal incontinence additionally endure from urinary incontinence. The majority of incontinence is a results of obstetric harm to the pelvic floor, either while carrying a fetus or in the course of the supply. Risk factors at the time of delivery embrace prolonged labor, the use of forceps, and the need for an episiotomy. Symptoms of incontinence can present after two or extra a long time following obstetric injury. Medical circumstances recognized to contribute to the event of fecal incontinence are listed in Table 353-4. Anatomy and Pathophysiology the anal sphincter complex is made up of the internal and exterior anal sphincter. The inner sphincter is clean muscle and a continuation of the round fibers of the rectal wall. It is innervated by the intestinal myenteric plexus and is subsequently not underneath voluntary management. The exterior anal sphincter is formed in continuation with the levator ani muscle tissue and is beneath voluntary management. Obstetric injury could end in tearing of the muscle fibers anteriorly on the time of the delivery. Injury may also be the results of stretching of the pudendal nerves during being pregnant or delivery of the fetus by way of the start canal. Presentation and Evaluation Patients may undergo with varying degrees of fecal incontinence. Minor incontinence includes incontinence to flatus and occasional seepage of liquid stool. For this cause, quality-of-life measures are an important component within the analysis of sufferers with fecal incontinence. Centers that take care of sufferers with fecal incontinence could have an anorectal physiology laboratory that makes use of standardized methods of evaluating anorectal physiology. Finally, endoanal ultrasound will consider the extent of the harm to the sphincter muscular tissues earlier than surgical restore. Unfortunately, all of those investigations are user-dependent, and only a few research demonstrate that these research predict outcome following an intervention. The majority of patients with fecal incontinence may have some extent of urinary incontinence. The results have been promising, with over 50% reaching larger than 50% reduction in incontinence episodes, and these outcomes have been sustainable as a lot as 2 years. This technique is another much less invasive therapy for sufferers with fecal incontinence. Radiofrequency power delivery to the anal canal in sufferers with fecal incontinence aids in the growth and restructuring of collagen fibers and supplies tensile energy to the sphincter muscular tissues. The outcomes have been variable, with 20�50% of patients having a sustained discount in incontinence episodes for 5 years. Finally, the utilization of stem cells to improve the majority of the sphincter muscle tissue is at present being tested. The typical low-fiber, high-fat Western food regimen is related to constipation and straining and the event of symptomatic hemorrhoids. Anatomy and Pathophysiology Hemorrhoidal cushions are a normal a part of the anal canal. Three major hemorrhoidal complexes traverse the anal canal-the left lateral, the best anterior, and the best posterior. External hemorrhoids originate beneath the dentate line and are coated with squamous epithelium and are associated with an inside part. Internal hemorrhoids originate above the dentate line and are lined with mucosa and transitional zone epithelium and characterize majority of hemorrhoids. The normal classification of hemorrhoidal disease is predicated on the development of the illness from their normal internal location to the prolapsing exterior position (Table 353-5). Presentation and Evaluation Patients generally current to a physician for 2 reasons: bleeding and protrusion. These include fiber supplementation, loperamide, diphenoxylate, and bile acid binders. These brokers harden the stool and delay frequency of bowel movements and are helpful in patients with minimal to mild signs. Furthermore, sufferers may be provided a form of physical therapy referred to as biofeedback. This therapy helps strengthen the exterior sphincter muscle while training the patient to chill out with defecation to avoid unnecessary straining and additional damage to the sphincter muscles. Biofeedback has had variable success and is dependent on the motivation of the affected person. For this cause, it must be integrated into the initial advice to all sufferers with fecal incontinence. The "gold standard" for the treatment of fecal incontinence with an isolated sphincter defect has been the overlapping sphincteroplasty. The exterior anal sphincter muscle and scar tissue in addition to any identifiable inside sphincter muscle are dissected free from the encompassing adipose and connective tissue and then an overlapping restore is performed in an try and rebuild the muscular ring and restore its function. Long-term outcomes following overlapping sphincteroplasty show a couple of 50% failure price over 5 years. Poorer end result has been seen in patients with prolonged pudendal nerve terminal motor latency. Sacral neuromodulation, collagen-enhancing injectables, radiofrequency remedy, and the artificial bowel sphincter are different options.
Syndromes
- Muscle pain (especially muscle pain with breathing, chewing, or using large muscles)
- Bone infections (osteomyelitis) that have not improved with other treatments
- If you have heart disease or you are older, your doctor may start you on a very small dose.
- Serum glucagon
- Burns
- Infection (a slight risk any time the skin is broken)
- Easy fatigue
- Feel liquid, firm, or solid
- Liver infection (hepatitis)
Periactin 4mg
As lactose digestion is rate-limiting compared to allergy testing okc generic periactin 4mg with amex glucose/galactose absorption allergy testing accuracy cheap periactin 4 mg overnight delivery, lactase deficiency is related to vital lactose malabsorption allergy testing mayo clinic periactin 4 mg with amex. Some people with lactose malabsorption develop signs such as diarrhea, belly ache, cramps, and/or flatus. The growth of signs of lactose intolerance is expounded to several elements: 1. Therefore, skim milk is extra likely to be associated with symptoms of lactose intolerance than entire milk, as the speed of gastric emptying after skim milk consumption is extra fast. Similarly, diarrhea following subtotal gastrectomy is often a result of lactose intolerance, as gastric emptying is accelerated in sufferers with a gastrojejunostomy. For instance, a clinician evaluating a patient who has symptoms suggestive of malabsorption and who has lately undergone in depth small-intestinal resection for mesenteric ischemia ought to direct the initial assessment almost completely to defining whether a short-bowel syndrome may explain the entire medical image. Similarly, the event of a sample of bowel actions suggestive of steatorrhea in a patient with long-standing alcohol abuse and continual pancreatitis ought to prompt an assessment of pancreatic exocrine function. Dietary nutrient absorption could additionally be segmental or diffuse along the small intestine and is site specific. Thus, for instance, calcium, iron, and folic acid are solely absorbed by active-transport processes within the proximal small intestine, particularly the duodenum; in distinction, the active-transport mechanisms for both cobalamin and bile acids are operative solely in the ileum. However, after segmental resection of the small gut, the remaining segments bear both morphologic and useful "adaptation" to enhance absorption. Such adaptation is secondary to the presence of luminal nutrients and hormonal stimuli and is in all probability not complete in humans for a number of months after resection. Establishing the diagnosis of steatorrhea and figuring out its specific cause are sometimes fairly tough. From a sensible standpoint, stool collections are invariably troublesome and infrequently incomplete, as no person desires to deal with stool. Additional research embrace measurement of serum carotene, ldl cholesterol, albumin, iron, folate, and cobalamin levels. If steatorrhea and/or altered absorption of different vitamins is suspected, then history, clinical observations, and laboratory testing may help detect deficiency of a nutrient, especially of a fat-soluble vitamin (A, D, E, or K). Thus, proof of metabolic bone illness with elevated alkaline phosphatase concentrations and/or reduced serum calcium ranges suggests vitamin D malabsorption. Macrocytic anemia leads to an analysis for possible cobalamin or folic acid malabsorption. Iron-deficiency anemia in the absence of occult bleeding from the gastrointestinal tract in either a male patient or a nonmenstruating feminine patient requires an evaluation for iron malabsorption and the exclusion of celiac disease, as iron is absorbed solely within the proximal small gut. At instances, nevertheless, a timed (72-h) quantitative stool assortment, preferably while the affected person is on a defined food regimen, must be undertaken so as to determine stool fats content and set up the diagnosis of steatorrhea. The presence of steatorrhea then requires additional evaluation to identify the pathophysiologic process(es) liable for the defect in dietary lipid digestion/absorption (Table 349-4). An understanding of the physiology and pathophysiology of cobalamin absorption may be very valuable, enhancing comprehension of elements of gastric, pancreatic, and ileal function. The d-xylose take a look at is normally performed by administering 25 g of d-xylose and amassing urine for five h. The d-xylose take a look at can be irregular in sufferers with blind loop syndrome (as a consequence primarily of an irregular intestinal mucosa) and, as a false-positive research, in sufferers with large collections of fluid in a 3rd space. The ease of obtaining a mucosal biopsy of the small intestine by endoscopy and the false-negative rate of the d-xylose check have led to its diminished use. When small-intestinal mucosal disease is suspected, a small-intestinal mucosal biopsy ought to be carried out. This examine is most frequently carried out along side an examination of the esophagus, abdomen, and duodenal bulb. Because inadequate barium is given to the affected person to allow an adequate examination of the small-intestinal mucosa, especially within the ileum, many gastrointestinal radiologists alter the procedure by performing either a small-bowel collection during which a large amount of barium is given by mouth, with out concurrent examination of the esophagus and stomach, or an enteroclysis study by which a great amount of barium is launched into the duodenum by way of a fluoroscopically positioned tube. Nonetheless, in skilled hands, barium contrast examination of the small gut can yield important info. For example, with intensive mucosal disease, intestinal dilation may be seen as a dilution of barium from increased intestinal fluid secretion. Capsule endoscopy and double-balloon enteroscopy are other helpful aids in the diagnostic evaluation of small-intestinal pathology. The main indications for a small-intestinal biopsy are analysis of a patient (1) both with documented or suspected steatorrhea or with continual diarrhea, and (2) with diffuse or focal abnormalities of the small gut outlined on a small-intestinal sequence. Lesions seen on small-bowel biopsy could be categorised into three categories (Table 349-6): 1. Relatively few ailments related to altered nutrient absorption have specific histopathologic abnormalities on small-intestinal mucosal biopsy, and these illnesses are uncommon. Abetalipoproteinemia is characterised by a traditional mucosal look apart from the presence of mucosal absorptive cells that comprise lipid postprandially and disappear after a chronic period of both fat-free intake or fasting. The attribute feature is the absence of or substantial reduction within the variety of plasma cells within the lamina propria; the mucosal structure could additionally be either completely regular or flat. Several diseases feature an irregular small-intestinal mucosa with a patchy distribution. As a outcome, biopsy samples obtained randomly or within the absence of endoscopically visualized abnormalities might not reveal diagnostic options. Intestinal lymphoma can at instances be diagnosed on mucosal biopsy by the identification of malignant lymphoma cells in the lamina propria and submucosa (Chap. Dilated lymphatics in the submucosa and sometimes in the lamina propria point out lymphangiectasia associated with hypoproteinemia secondary to protein loss into the gut. Eosinophilic gastroenteritis includes a heterogeneous group of disorders with a spectrum of shows and symptoms, with an eosinophilic infiltrate of the lamina propria, and with or with out peripheral eosinophilia. The patchy nature of the infiltrate and its presence within the submucosa usually result in an absence of histopathologic findings on mucosal biopsy. Amyloid deposition may be identified by Congo Red staining in some sufferers with amyloidosis involving the duodenum (Chap. The analysis of celiac illness is established by scientific, histologic, and immunologic responses to a gluten-free diet. Celiac illness has had several other names, together with nontropical sprue, celiac sprue, adult celiac illness, and gluten-sensitive enteropathy. A small number of individuals have classical signs and manifestations related to nutrient malabsorption along with a various pure historical past; the onset of signs can occur at all points from the primary 12 months of life through the eighth decade. The histologic adjustments have a proximal-to-distal intestinal distribution of severity, which probably displays the exposure of the intestinal mucosa to varied quantities of dietary gluten. The signs range from important malabsorption of multiple nutrients, with diarrhea, steatorrhea, weight loss, and the implications of nutrient depletion. Asymptomatic relations of patients with celiac disease have been identified as having this disease either by small-intestinal biopsy or by serologic studies. The availability of these "celiac serologies" has led to a considerable increase in the frequency of analysis of celiac disease, and the prognosis is now being made primarily in sufferers with out "classic" signs but with atypical and subclinical shows.
Discount periactin 4mg otc
Gastrointestinal prophylaxis with proton pump inhibitors or histamine (H2) receptor blockers is required allergy testing dogs buy generic periactin 4 mg. On the other hand allergy medicine active ingredient generic periactin 4mg on-line, initiating dialysis too early might unnecessarily expose people to intravenous traces and invasive procedures allergy symptoms yeast buy periactin 4 mg visa, with the attendant dangers of infection, bleeding, procedural issues, and hypotension. Ureteric obstruction could additionally be handled by percutaneous nephrostomy tube placement or ureteral stent placement. In uncommon instances, extreme polyuria persists because of tubular dysfunction and will require continued administration of intravenous fluids and electrolytes for a time frame. In severe instances of quantity overload, furosemide could additionally be given as a bolus (200 mg) adopted by an intravenous drip (10�40 mg/h), with or with no thiazide diuretic. In decompensated coronary heart failure, stepped diuretic remedy was discovered to be superior to ultrafiltration in preserving gradient ("diffusive" clearance) and/or together with the movement of plasma water ("convective" clearance). The selection of modality is usually dictated by the quick availability of know-how and the experience of medical staff. Dialysate resolution is instilled into and removed from the peritoneal cavity at common intervals so as to achieve diffusive and convective clearance of solutes throughout the peritoneal membrane; ultrafiltration of water is achieved by the presence of an osmotic gradient throughout the peritoneal membrane achieved by high concentrations of dextrose in the dialysate resolution. Peritoneal dialysis is probably not enough for hypercatabolic patients because of inherent limitations in dialysis efficacy. Hemodialysis can be used intermittently or continuously and may be accomplished by way of convective clearance, diffusive clearance, or a mixture of the 2. Hemodialysis is an intermittent process that removes solutes via diffusive and convective clearance. However, the risk of worsening of kidney function is carefully linked to the amount of albuminuria, and so it has been included into the classification. This syndrome leads to death until the toxins are removed by renal replacement remedy, using dialysis or kidney transplantation. The responses to discount in nephron number are mediated by vasoactive hormones, cytokines, and growth factors. Eventually, these short-term variations of hypertrophy and hyperfiltration become maladaptive because the increased pressure and circulate within the nephron predisposes to distortion of glomerular structure, abnormal podocyte function, and disruption of the filtration barrier resulting in sclerosis and dropout of the remaining nephrons. This process explains why a reduction in renal mass from an isolated insult might result in a progressive decline in renal function over a few years. Risk elements embrace small for gestation delivery weight, childhood obesity, hypertension, diabetes mellitus, autoimmune illness, advanced age, African ancestry, a family history of kidney disease, a earlier episode of acute kidney harm, and the presence of proteinuria, irregular urinary sediment, or structural abnormalities of the urinary tract. In addition, latest analysis within the genetics of predisposition to common complicated illnesses (Chap. The prevalence in West African populations seems to have arisen as an evolutionary adaptation conferring protection from tropical pathogens. However, the overwhelming majority of these patients will present no further deterioration of renal operate. The first contains sufferers with a silent primary glomerulopathy, corresponding to focal segmental glomerulosclerosis, with out the overt nephrotic or nephritic manifestations of glomerular disease (Chap. The second includes sufferers in whom progressive nephrosclerosis and hypertension is the renal correlate of a systemic vascular illness, often also involving large- and small-vessel cardiac and cerebral pathology. Right: Low-power photomicrograph of continual kidney disease with sclerosis of many glomeruli and extreme tubulointerstitial fibrosis (Masson trichrome, �40 magnification). Although an correct 24-h urine assortment is the usual for measurement of albuminuria, the measurement of protein-to-creatinine ratio in a spot first-morning urine sample is often extra sensible to get hold of and correlates nicely, but not completely, with 24-h urine collections. It is a good screening test for early detection of renal illness, and could also be a marker for the presence of microvascular disease generally. A host of metabolic and endocrine capabilities normally performed by the kidneys can be impaired or suppressed, and this ends in anemia, malnutrition, and irregular metabolism of carbohydrates, fat, and proteins. In abstract, the pathophysiology of the uremic syndrome may be divided into manifestations in three spheres of dysfunction: (1) these consequent to the accumulation of toxins that normally undergo renal excretion, together with products of protein metabolism; (2) these consequent to the lack of other kidney functions, such as fluid and electrolyte homeostasis and hormone regulation; and (3) progressive systemic inflammation and its vascular and dietary consequences. Notwithstanding these two homeostatic responses, hyperkalemia may be precipitated in sure settings. These embrace increased dietary potassium consumption, protein catabolism, hemolysis, hemorrhage, transfusion of stored red blood cells, and metabolic acidosis. In addition, a number of medications can inhibit renal potassium excretion and result in hyperkalemia. These embody conditions related to hyporeninemic hypoaldosteronism, corresponding to diabetes, and renal ailments that preferentially affect the distal nephron, similar to obstructive uropathy and sickle cell nephropathy. The concomitant sodium load mandates cautious consideration to quantity status and the necessity for diuretic agents. With regular renal function, the tubular reabsorption of filtered sodium and water is adjusted in order that urinary excretion matches intake. The rare affected person with salt-losing nephropathy might require a sodiumrich diet or salt supplementation. It is likely that problems of bone turnover and issues of vascular and delicate tissue calcification are associated to one another. This affected person was on hemodialysis for many years and was nonadherent to dietary phosphorus restriction or using phosphate binders. Clinical manifestations of extreme hyperparathyroidism include bone ache and fragility, brown tumors, compression syndromes, and erythropoietin resistance partially associated to the bone marrow fibrosis. Low-turnover bone illness could be grouped into two categories- adynamic bone disease and osteomalacia. Adynamic bone disease is rising in prevalence, particularly amongst diabetics and the elderly. Occasionally the calcium will precipitate within the delicate tissues into large concretions termed "tumoral calcinosis". Finally, hyperphosphatemia can induce a change in gene expression in vascular cells to an osteoblast-like profile, resulting in vascular calcification and even ossification. Recognition of the role of the extracellular calcium-sensing receptor has led to the development of calcimimetic agents that improve the sensitivity of the parathyroid cell to the suppressive effect of calcium. Traditional risk components embody hypertension, hypervolemia, dyslipidemia, sympathetic overactivity, and hyperhomocysteinemia. The inflammatory state related to a reduction in kidney perform is reflected in increased circulating acute-phase reactants, similar to inflammatory cytokines and C-reactive protein, with a corresponding fall in the "unfavorable acute-phase reactants," such as serum albumin and fetuin. This peritoneal dialysis patient was on persistent warfarin remedy for atrial fibrillation. She noticed a small painful nodule on the abdomen that was followed by progressive pores and skin necrosis and ulceration of the anterior belly wall. She was handled with hyperbaric oxygen, intravenous thiosulfate, and discontinuation of warfarin, with gradual resolution of the ulceration. It is heralded by livedo reticularis and advances to patches of ischemic necrosis, particularly on the legs, thighs, stomach, and breasts. A major aspect impact of calcium-based phosphate binders is calcium accumulation and hypercalcemia, particularly in sufferers with low-turnover bone disease. In addition, hemodialysis, with its attendant episodes of hypotension and hypovolemia, could additional worsen coronary ischemia and repeatedly stun the myocardium. Therefore, the development in levels over the hours after presentation may be extra informative than a single, elevated degree.
Buy 4 mg periactin with mastercard
Only the vagal fibers innervating the portion of the abdomen that incorporates parietal cells is transected allergy treatment epipen purchase periactin 4 mg amex, thus leaving fibers important for regulating gastric motility intact allergy symptoms from grass cheap periactin 4mg amex. By the end of the first postoperative 12 months allergy shots ok during pregnancy purchase periactin 4 mg on-line, basal and stimulated acid output are ~30 and 50%, respectively, of preoperative levels. Ulcer recurrence rates are larger 1925 with highly selective vagotomy (10%), although the overall complication charges are the bottom of the three procedures. Antrectomy is geared toward eliminating an additional stimulant of gastric acid secretion, gastrin. Selection of vagotomy and antrectomy may be more applicable in these circumstances. The creation of laparoscopic surgery has led a number of surgical teams to successfully carry out highly selective vagotomy, truncal vagotomy/pyloroplasty, and truncal vagotomy/antrectomy via this method. Morbidity associated with vagotomy and antrectomy or pyloroplasty is 5%, with mortality ~1%. In addition to the potential early penalties of any intraabdominal process (bleeding, an infection, thromboembolism), gastroparesis, duodenal stump leak, and efferent loop obstruction can be observed. Ulcers may recur for several reasons, including incomplete vagotomy, inadequate drainage, retained antrum, and, much less likely, persistent or recurrent H. Incomplete vagotomy could be ruled out by gastric acid evaluation coupled with sham feeding. An improve in gastric acid output in response to sham feeding is proof that the vagus nerve is undamaged. A rise in serum pancreatic polypeptide >50% within 30 min of sham feeding can additionally be suggestive of an intact vagus nerve. These signs and symptoms come up from the fast emptying of hyperosmolar gastric contents into the small gut, leading to a fluid shift into the gut lumen with plasma volume contraction and acute intestinal distention. Up to 50% of postvagotomy and drainage sufferers will experience dumping syndrome to some degree early on. Signs and signs often enhance with time, however a extreme protracted picture can occur in up to 1% of sufferers. The somatostatin analogue octreotide has been successful in diet-refractory circumstances. This drug is administered subcutaneously (50 g tid), titrated in accordance with medical response. A long-acting depot formulation of octreotide may be administered as soon as each 28 days and provides symptom reduction similar to the short-acting agent. This complication is most commonly observed after truncal vagotomy, which is rarely carried out right now. Patients may complain of intermittent diarrhea that occurs usually 1�2 h after meals. Other contributing components might embody decreased absorption of vitamins (see below), increased excretion of bile acids, and launch of luminal components that promote secretion. Surgical reversal of a 10-cm section of jejunum may yield a considerable enchancment in bowel frequency in a subset of sufferers. Histologic examination of the gastric mucosa reveals minimal inflammation however the presence of epithelial cell damage. The extra common of the two is bacterial overgrowth in the afferent limb secondary to stasis. Pain is often followed by nausea and vomiting of reason for this disorder, the mechanism is unknown. Prokinetic brokers, cholestyramine, and sucralfate have been considerably effective remedies. Bilious vomiting improves, however early satiety and bloating may persist in up to 50% of patients. Patients can experience a 10% loss of body weight, which stabilizes 3 months postoperatively. Reasons for maldigestion/malabsorption embrace decreased gastric acid manufacturing, speedy gastric emptying, decreased meals dispersion in the abdomen, lowered luminal bile concentration, lowered pancreatic secretory response to feeding, and rapid intestinal transit. Osteomalacia can happen as a late complication in up to 25% of post�partial gastrectomy sufferers. Elevated alkaline phosphatase, reduced serum calcium, bone ache, and pathologic fractures may be seen in sufferers with osteomalacia. Copper deficiency has also been reported in patients present process surgeries that bypass the duodenum, where copper is primarily absorbed. Patients may current with a uncommon syndrome that features ataxia, myelopathy, and peripheral neuropathy. Gastric aDenocarcinoma the incidence of adenocarcinoma within the gastric stump is elevated 15 years after resection. Some have reported a four- to fivefold increase in gastric cancer 20�25 years after resection. The pathogenesis is unclear however could contain alkaline reflux, bacterial proliferation, or hypochlorhydria. The latter is assumed to be due to decreased gallbladder contractility related to vagotomy and bypass of the duodenum, leading to decreased postprandial launch of cholecystokinin. Males are more generally affected than females, and nearly all of patients are recognized between ages 30 and 50. Longstanding hypergastrinemia results in markedly increased gastric acid secretion through both parietal cell stimulation and increased parietal cell mass. The increased gastric acid output leads to peptic ulcer diathesis, erosive esophagitis, and diarrhea. Tumor Distribution Although early research suggested that the overwhelming majority of gastrinomas occurred throughout the pancreas, a major number of these lesions are extrapancreatic. Duodenal tumors constitute the most common nonpancreatic lesion; between 50 and 75% of gastrinomas are found here. Less common extrapancreatic websites include stomach, bones, ovaries, coronary heart, liver, and lymph nodes. More than 60% of tumors are thought of malignant, with as a lot as 30�50% of patients having a number of lesions or metastatic illness at presentation. Histologically, gastrin-producing cells seem well-differentiated, expressing markers usually found in endocrine neoplasms (chromogranin, neuron-specific enolase). Clinical situations that ought to create suspicion of gastrinoma are ulcers in unusual locations (second a half of the duodenum and beyond), ulcers refractory to commonplace medical therapy, ulcer recurrence after acid-reducing surgical procedure, ulcers presenting with frank issues (bleeding, obstruction, and perforation), or ulcers within the absence of H. Diarrhea, the subsequent most common medical manifestation, is found in up to 50% of patients. Although diarrhea often happens concomitantly with acid peptic disease, it may additionally occur impartial of an ulcer. Etiology of the diarrhea is multifactorial, resulting from marked quantity overload to the small bowel, pancreatic enzyme inactivation by acid, and injury of the intestinal epithelial floor by acid. The epithelial damage can lead to a light diploma of maldigestion and malabsorption of vitamins. The diarrhea may have a secretory element due to the direct stimulatory impact of gastrin on enterocytes or the co-secretion of further hormones from the tumor corresponding to vasoactive intestinal peptide.
Discount periactin 4 mg with mastercard
If left untreated allergy yeast symptoms rash buy periactin 4mg without a prescription, early mucosal stress ulceration will progress to fullthickness damage allergy medicine in 3rd trimester purchase periactin 4 mg without prescription. An overview of analysis and management of each type of intestinal ischemia is given in Table 354-1 allergy testing environmental cheap 4 mg periactin with visa. Associated symptoms might embrace nausea and vomiting, transient diarrhea, anorexia, and bloody stools. With the exception of minimal belly distention and hypoactive bowel sounds, early belly examination is unimpressive. In the evaluation of acute intestinal ischemia, routine laboratory tests should be obtained, including full blood count, serum chemistry, coagulation profile, arterial blood gasoline, amylase, lipase, lactic acid, blood sort and cross match, and cardiac enzymes. Often the decision to operate is made on a excessive index of suspicion from the history and physical exam regardless of normal laboratory findings. More just lately, mesentery duplex scanning and visual mild spectroscopy throughout colonoscopy have been demonstrated to be useful. A plain abdominal film could show evidence of free intraperitoneal air, indicating a perforated viscus and the necessity for emergent exploration. Earlier options of intestinal ischemia seen on abdominal radiographs embody bowel-wall edema, often known as "thumbprinting. Other features embody calcifications of the aorta and its tributaries, indicating atherosclerotic illness. The biggest limitation of duplex scanning is body habitus; in overweight patients, imaging is poor yield. However, in sufferers with chronic illness, "food fear" usually leads to a decreased urge for food and therefore much less belly fats, and duplex imaging may be very high yield. The endoscopic strategies utilizing seen mild spectroscopy can be used in the prognosis of continual ischemia. The "gold standard" for the diagnosis of acute arterial occlusive illness is angiography, and administration is laparotomy. The complete size of the small and huge bowel starting on the ligament of Treitz should be evaluated. The surgical administration of acute mesenteric ischemia of the small bowel is embolectomy via arteriotomy; a small incision is made in the artery by way of which the clot is retrieved. Another method to handle acute thrombosis is thrombolysis therapy and angioplasty, with stent placement. However, this method is more generally utilized to treat persistent mesenteric ischemia. Nonocclusive or vasospastic mesenteric ischemia presents with generalized stomach ache, anorexia, bloody stools, and stomach distention. Often these patients are obtunded, and physical findings could not help in the analysis. The presence of a leukocytosis, metabolic acidosis, elevated amylase or creatinine phosphokinase ranges, and/or lactic acidosis is useful in assist of the prognosis of advanced intestinal ischemia; however, these markers is probably not indicative of either reversible ischemia or frank necrosis. Regardless of the need for urgent surgical procedure, emergent admission to a monitored mattress or intensive care unit is beneficial for resuscitation and further evaluation. Early manifestations of intestinal ischemia embody fluid sequestration inside the bowel wall leading to a loss of interstitial volume. Broadspectrum antibiotics must be given to provide enough coverage for enteric pathogens, together with gram-negative and anaerobic organisms. All vasoconstricting agents ought to be avoided; fluid resuscitation is the intervention of choice to preserve hemodynamics. If ischemic colitis is a concern, colonoscopy must be carried out to assess the integrity of the colon mucosa. Visualization of the rectosigmoid area could reveal decreased mucosal integrity, associated extra commonly with nonocclusive mesenteric ischemia, or, every so often, occlusive illness as a end result of acute lack of inferior mesenteric arterial move following aortic surgery. Ischemia of the colonic mucosa is graded as gentle with minimal mucosal erythema or as reasonable with pale mucosal ulcerations and proof of extension to the muscular layer of the bowel wall. Severe ischemic colitis presents with severe ulcerations resulting in black or green discoloration of the mucosa, in preserving with full-thickness bowel-wall necrosis. The degree of reversibility could be predicted from the mucosal findings: delicate erythema is almost 100% reversible, moderate is roughly 50% reversible, and frank necrosis is just dead bowel. Follow-up colonoscopy could be carried out to rule out development of ischemic colitis. Ischemic colitis is optimally treated with resection of the ischemic bowel and formation of a proximal stoma. Patients with mesenteric venous thrombosis may present with a gradual or sudden onset. Intravenous distinction will demonstrate a delayed arterial part and clot within the superior mesenteric vein. If laparotomy is performed and mesenteric venous thrombosis is suspected, heparin anticoagulation is immediately initiated, and compromised bowel is resected. Of all acute intestinal issues, mesenteric venous insufficiency is related to the most effective prognosis. Chronic intestinal ischemia presents with intestinal angina or postprandial stomach pain related to need for increased blood flow to the gut following meals. Physical examination will usually reveal a malnourished patient with an stomach bruit as nicely as other manifestations of atherosclerosis. It is necessary to perform the check fasting as a end result of the presence of elevated bowel fuel prevents adequate visualization of move disturbances within the vessels or the lack of a vasodilation response to feeding during the test. This tool is frequently used as a screening test for sufferers with symptoms suggestive of persistent mesenteric ischemia. The gold standard for affirmation of mesenteric arterial occlusion is mesenteric angiography. Evaluation with mesenteric angiography permits for identification and attainable intervention for the treatment of atherosclerosis within the vessel lumen and will also evaluate the patency of remaining mesenteric vessels. Magnetic resonance angiography is another if the administration of contrast dye is contraindicated. The management of chronic intestinal ischemia includes medical administration of atherosclerotic disease by train, cessation of smoking, and antiplatelet and lipid-lowering medicines. A full cardiac evaluation should be performed before intervention on chronic mesenteric ischemia. Angioplasty with endovascular stenting in the therapy of persistent mesenteric ischemia is associated with an 80% long-term success price. In sufferers requiring surgical exploration, the approach used is set by findings of the mesenteric angiogram. Restoration of blood circulate on the time of laparotomy is accomplished with mesenteric vessel endarterectomy or bypass. Determination of intestinal viability intraoperatively in sufferers with suspected intestinal ischemia can be difficult. Palpation of major arterial mesenteric vessels could be performed, in addition to making use of a Doppler flowmeter to the antimesenteric border of the bowel wall, but neither is a definitive indicator of viability. If doubt persists, reexploration performed 24�48 h following surgical procedure will allow demarcation of nonviable bowel.
4mg periactin with amex
The percentage of deaths from these causes has been slowly rising because the numbers of transplanted diabetic patients and the common age of all recipients improve allergy shots not effective discount 4 mg periactin visa. More than 50% of renal recipient mortality is attributable to heart problems allergy symptoms contagious generic periactin 4mg without a prescription. In addition to strict control of blood pressure and blood lipid levels allergy testing houston cost discount 4mg periactin overnight delivery, shut monitoring of sufferers for indications of further medical or surgical intervention is a vital part of administration. Hypertension may be brought on by (1) native kidney illness, (2) rejection activity in the transplant, (3) renal artery stenosis if an end-to-end anastomosis was constructed with an iliac artery department, and (4) renal calcineurin inhibitor toxicity, which may enhance with reduction in dose. Amelioration of hypertension to the range of 120�130/70�80 mmHg ought to be the aim in all patients. Hypercalcemia after transplantation may indicate failure of hyperplastic parathyroid glands to regress. Aseptic necrosis of the top of the femur is probably as a result of preexisting hyperparathyroidism, with aggravation by glucocorticoid therapy. Although most transplant sufferers have strong production of erythropoietin and normalization of hemoglobin, anemia is usually seen within the posttransplant interval. Chronic hepatitis, notably when due to hepatitis B virus, can be a progressive, deadly illness over a decade or so. The dangers are elevated in proportion to the total immunosuppressive load administered and the time elapsed since transplantation. The glomerular capillary tuft derives from an afferent arteriole that types a branching capillary mattress embedded in mesangial matrix. This capillary network funnels into an efferent arteriole, which passes filtered blood into cortical peritubular capillaries or medullary vasa recta that supply and exchange with a folded tubular structure. Hence the glomerular capillary tuft, fed and drained by arterioles, represents an arteriolar portal system. Delicate foot processes extending from epithelial podocytes shroud the outer surface of those capillaries, and podocytes interconnect to one another by slitpore membranes forming a selective filtration barrier. The glomerular capillaries form from a branching community of renal arteries, arterioles, resulting in an afferent arteriole, glomerular capillary mattress (tuft), and a draining efferent arteriole. The mechanics of filtration and reclamation are fairly sophisticated for lots of solutes (Chap. For example, within the case of serum albumin, the glomerulus is an imperfect barrier. Remarkably, humans with normal nephrons excrete on common 8�10 mg of albumin in daily voided urine, approximately 20�60% of complete excreted protein. This quantity of albumin, and different proteins, can rise to gram portions following glomerular harm. The breadth of diseases affecting the glomerulus is expansive because the glomerular capillaries may be injured in quite lots of ways, producing many different lesions. Some order to this vast topic is introduced by grouping all of those ailments right into a smaller number of scientific syndromes. Systemic hypertension and atherosclerosis can produce pressure stress, ischemia, or lipid oxidants that result in persistent glomerulosclerosis. Malignant hypertension can rapidly complicate glomerulosclerosis with fibrinoid necrosis of arterioles and glomeruli, thrombotic microangiopathy, and acute renal failure. Most glomerular or mesangial antigens involved in immunemediated glomerulonephritis are unknown. Specific or distinctive features of pathogenesis are talked about with the outline of each of the glomerular diseases later in this chapter. Local activation of Toll-like receptors on glomerular cells, deposition of immune complexes, or complement damage to glomerular buildings induces mononuclear cell infiltration, which subsequently results in an adaptive immune response attracted to the kidney by local release of chemokines. While the adaptive immune response is just like that of other tissues, early T cell activation performs an essential function within the mechanism of glomerulonephritis. Amplification mediators as locally derived oxidants and proteases expand this irritation, and, relying on the situation of the goal antigen and the genetic polymorphisms of the host, basement membranes are damaged with both endocapillary or extracapillary proliferation. Immune deposits in the glomerular mesangium may end result from the deposition of preformed circulating complexes or in situ antigenantibody interactions. Immune deposits stimulate the discharge of local proteases and activate the complement cascade, producing C5�9 attack complexes. Overlapping etiologies or pathophysiologic mechanisms can produce comparable glomerular lesions, suggesting that downstream molecular and mobile responses usually converge toward frequent patterns of damage. The easiest explanation is that urine move is impeded by tubular obstruction because of interstitial irritation and fibrosis. Thus, obstruction of the tubules with debris or by extrinsic compression leads to aglomerular nephrons. A second mechanism means that interstitial changes, together with interstitial edema or fibrosis, alter tubular and vascular architecture and thereby compromise the normal tubular transport of solutes and water from tubular lumen to vascular area. This failure increases the solute and water content material of the tubule fluid, resulting in isosthenuria and polyuria. Adaptive mechanisms associated to tubuloglomerular feedback also fail, leading to a discount of renin output from the juxtaglomerular apparatus trapped by interstitial irritation. The cross-sectional volume of these capillaries is decreased by interstitial inflammation, edema, or fibrosis. These structural alterations in vascular resistance have an effect on renal perform via two mechanisms. First, tubular cells are very metabolically active, and, consequently, decreased perfusion results in ischemic injury. Second, impairment of glomerular arteriolar outflow results in elevated intraglomerular hypertension in less-involved glomeruli; this selective intraglomerular hypertension aggravates and extends mesangial sclerosis and glomerulosclerosis to less-involved glomeruli. Persistent harm to glomerular capillaries spreads to the tubulointerstitium in association with proteinuria. There is a speculation that efferent arterioles main from inflamed glomeruli carry ahead inflammatory mediators, which induces downstream interstitial nephritis, leading to fibrosis. The simplest explanation for the impact of proteinuria on the development of interstitial nephritis is that more and more severe proteinuria, carrying activated cytokines and lipoproteins producing reactive oxygen species, triggers a downstream inflammatory cascade in and round epithelial cells lining the tubular nephron. These effects induce T lymphocyte and macrophage infiltrates within the interstitial areas along with fibrosis and tubular atrophy. In experimental studies, bone morphogenetic protein 7 and hepatocyte growth factor can reverse early fibrogenesis and preserve tubular structure. When fibroblasts outdistance their survival elements, apoptoses happens, and the everlasting renal scar becomes acellular, leading to irreversible renal failure. As few as three to 5 red blood cells within the spun sediment from first-voided morning urine is suspicious. When working up microscopic hematuria, perhaps accompanied by minimal proteinuria (<500 mg/24 h), it could be very important exclude anatomic lesions, such as malignancy of the urinary tract, significantly in older men. Sustained proteinuria >1�2 g/24 h can be generally related to glomerular illness. Sustained proteinuria has to be distinguished from lesser amounts of so-called benign proteinuria in the regular inhabitants (Table 338-1).
References
- Khanna D, Gladue H, Channick R, et al. Recommendations for screening and detection of connective tissue disease-associated pulmonary arterial hypertension. Arthritis Rheum. 2013;65:3194-3201.
- Giardina EG, Heissenbuttel RH, Bigger JT Jr. Intermittent intravenous procaine amide to treat ventricular arrhythmias: correlation of plasma concentration with effect on arrhythmia, electrocardiogram, and blood pressure. Ann Intern Med 1973;78(2): 183-193.
- Stewart JT, McKenna WJ: Management of arrhythmias in hypertrophic cardiomyopathy, Cardiovasc Drugs Ther 8:95, 1994.
- Pally E, Kreder HJ. Survey of terminology used for the intraoperative direction of C-arm fluoroscopy. Can J Surg. 2013;56:109-112.