
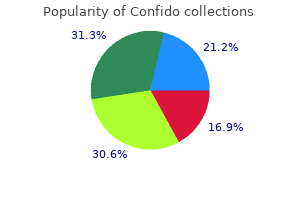
Confido
Carol A. Kauffman, M.D.
- Professor
- Department of Internal Medicine
- University of Michigan Medical School Chief
- Infectious Diseases Section
- Veterans Affairs Ann Arbor Healthcare System
- Ann Arbor, Michigan
Confido dosages: 60 caps
Confido packs: 1 bottles, 2 bottles, 3 bottles, 4 bottles, 5 bottles, 6 bottles, 7 bottles, 8 bottles, 9 bottles, 10 bottles

Order confido 60 caps with visa
This check identifies patients at elevated threat for ischemic complications from radial artery catheterization prostate help order confido 60 caps fast delivery. The procedure has undergone many modifications57 prostate cancer cure rate generic confido 60caps,58 since originally being described in a cooperative affected person prostate cancer 51 purchase confido 60caps with visa. The modified Allen take a look at is carried out as follows: occlude each the radial and ulnar arteries with digital stress and then ask the patient to tightly clench the fist repeatedly to exsanguinate the hand. After 2 minutes, repeat the take a look at in the same method with release of the radial artery only. Rubor should return quickly to the hand following the release of strain from either vessel. An irregular (positive) Allen check outcome, suggestive of inadequate collateralization, is defined as the continued presence of pallor 5 to 15 seconds after release of the radial artery. Be careful to keep away from overextension of the hand with broad separation of the digits, which can compress the palmar arches between fascial planes and yield a false-positive result. At the wrist, the radial artery rests on the flexor digitorum superficialis muscle, the flexor pollicis longus muscle, the pronator quadratus muscle, and the radius bone. In this location, it supplies a extra consistent site for cannulation because of its fixation and decreased mobility. Dorsiflexing the wrist at roughly a 45-degree angle over a towel or sandbag and fixing the wrist to an arm board will also help isolate the artery. Then, underneath direct vision, cannulation of the artery turns into as simple as venous cannulation. Release the ulnar artery and observe the hand for return of rubor, which signifies good move in the ulnar artery. If brisk filling occurs, repeat the take a look at with launch of the radial artery to assess radial artery patency. If each the radial and ulnar arteries show patency, the wrist could also be used for arterial cannulation. Before puncturing the radial artery for cannulation, it is necessary to identify a reliable ulnar artery ought to harm to the radial artery happen. At the wrist, the ulnar artery runs alongside the palmar margin of the flexor carpi ulnaris in the area between it and the flexor digitorum sublimis. Dorsalis Pedis Artery the dorsalis pedis artery continues from the anterior tibial artery and runs from roughly halfway between the malleoli to the posterior finish of the first metatarsal space, where it types the dorsal metatarsal and deep plantar arteries. The lateral plantar artery, a department of the posterior tibial artery, passes obliquely across the foot to the base of the fifth metatarsal. The plantar arch is accomplished on the point where the lateral plantar artery joins the deep plantar artery between the first and second metatarsals. On the dorsum of the foot, the dorsalis pedis artery lies in the subcutaneous tissue parallel to the extensor hallucis longus tendon and between it and the extensor digitorum longus. Although this vessel is amenable to cutdown, the vascular anatomy of the foot is quite variable. This is of no consequence if a pulse may be palpated, however Huber,73 in his dissection of 200 toes, noted that the dorsalis pedis artery was absent in 12% of sufferers. In 16% of patients the dorsalis pedis artery offered the principle blood supply to the toes. The strain wave obtained with an electronic transducer hooked up to the dorsalis pedis artery shall be 5 to 20 mm Hg higher than that of the radial artery and, as properly as, will be delayed by zero. The brachial artery begins because the continuation of the axillary artery and ends on the head of the radius, the place it splits into the ulnar and radial arteries. The most popular puncture website of the brachial artery is in or simply proximal to the antecubital fossa. In this region, the artery lies on top of the brachialis muscle and enters the fossa underneath the bicipital aponeurosis with the median nerve, and on the medial aspect of the artery. Both the radial and the axillary arteries are most well-liked over the brachial artery within the upper extremity. Nonetheless, safe cannulation of the brachial artery has been demonstrated by some investigators. A longer catheter (10 cm) is required for the brachial artery in order that sufficient length is out there to traverse the elbow joint. Femoral Artery the femoral artery is the second mostly used vessel for arterial cannulation. The femoral artery is the direct continuation of the iliac artery and enters the thigh after passing below the inguinal ligament. Arterial puncture should at all times happen distal to the ligament to prevent uncontrolled hemorrhage into the pelvis or peritoneum. The advantage of cannulating the artery at a website just distal to the inguinal ligament is that the artery could be compressed against the femoral head. Cannulation turns into tougher the more distal the puncture website is from the inguinal ligament as a result of the femoral artery splits into the superficial femoral and the deep femoral arteries. These arteries, particularly the deep femoral, may be challenging to compress if bleeding needs to be controlled. One method of finding an acceptable arterial puncture site is to place the thumb and fifth finger on the pubis symphysis and the anterior iliac backbone and find the artery beneath the center knuckle. When puncturing this vessel, watch out to avoid the femoral nerve and vein, which form the lateral and medial borders, respectively. A longer, larger-diameter catheter is required for correct monitoring of the femoral artery because of its measurement and the comparatively higher depth at which it lies. Only the Seldinger technique is beneficial for this site, which allows placement of a 15- to 20-cm plastic catheter for extended monitoring. Regardless of the device used, enter the skin with the needle at an angle of roughly 45 levels as a substitute of the standard 15 to 20 degrees. The extremely massive ratio of arterial diameter to catheter diameter is thought to scale back the incidence of thrombosis, particularly complete occlusion. However, occlusion has been reported with femoral cannulation for monitoring purposes. If the affected person is that mobile, rethink the risk-benefit ratio of invasive monitoring. Umbilical and Temporal Arteries In neonates, arterial entry could be achieved for a quick while by way of the umbilical artery (see Chapter 19). Because of the growing accuracy of ear oximeters and the use of capillary blood gas samples for dedication of pH, prolonged arterial cannulation will turn into less frequent throughout toddler care. Reported medical sequelae of arterial puncture and cannulation range from simple hematomas to life-threatening infections and exsanguination. In addition, ischemia, arteriovenous fistula, and pseudoaneurysm formation are attainable. It is troublesome to compare complication charges at varied sites because most printed studies have primarily used solely the radial artery. The most typical complication was vascular insufficiency (4%), adopted by bleeding (2. In a examine of 2400 consecutive cardiac catheterizations over a 12-month period, complications occurred in 1. The damage resulted from a failed try to place a proper femoral artery catheter via the Seldinger method.

Generic confido 60 caps on line
This represents a delay in closure of the aortic valve because of delayed left ventricular depolarization prostate oncology veterinarians buy confido 60caps with mastercard. In addition prostate questions and answers cheap 60caps confido free shipping, search for issues secondary to the process and deal with as needed mens health 8 week program cheap 60 caps confido otc. Catheter Placement in Low-Flow States If cardiac output is simply too low to float a pacing catheter or if the affected person is in extremis, there is most likely not sufficient time to advance a pacing catheter by way of the beforehand described methods. In such emergency situations, join the pacing catheter to the vitality source, turn the output to the utmost amperage, and select the asynchronous mode (see earlier section on Emergency Blind Passage). Rotate, advance, withdraw, or otherwise manipulate the pacing catheter in accordance with medical response. The proper inside jugular strategy is the most practical entry route on this scenario. One promising method includes using uS to help within the placement of emergency transvenous pacing catheters. The benefits of uS over fluoroscopy are: no exposure to ionizing radiation, lower charges of complications, and quicker occasions to pacemaker insertion. Testing Threshold the edge is the minimal present essential to acquire capture. If the threshold is in this perfect range, good contact with the endocardium can be presumed. Carry out this maneuver two or thrice to make certain that this worth is constant. Set the speed at roughly 10 beats/min greater than the endogenous rhythm, place the pacemaker in asynchronous mode (minimum sensitivity, which is the utmost setting on the sensitivity voltage control), and make positive that Complications the complications associated with emergency transvenous cardiac pacing are numerous and symbolize a compendium of these related to central venous catheterization,13,62 those related to right-sided heart catheterization, and people distinctive to the pacing catheter itself. Overall rates of adverse occasions using modern flexible, balloon-tipped catheters are within the vary of 20%. Additionally, ultrasound is helpful in attaining the central venous entry essential to introduce the pacemaker. In the absence of a phased-array or microconvex transducer, a curvilinear transducer may be adequate. If the transducer will be used near or on the sector, it could be positioned inside a sterile cover or a sterile glove. A hand must be placed on prime of the transducer to allow the sonographer to push downward into the epigastric space. The transducer can then be aimed towards the left facet of the chest till the four-chambered view of the heart is seen. Deep to that is the heart, with the proper atrium and ventricle abutting the liver. The right ventricle is seen through the subxiphoid window, which provides wonderful views of the heart with out interfering with placement of the pacemaker line. The pacemaker wire is seen as a brightly echogenic structure within the proper ventricle. Once the pacer wire has been inserted, the sonographer should start observing the proper atrium. The wire will appear as a hyperechoic (white) linear echo because it enters the proper atrium and it can be seen to advance in actual time. Capture of the pacemaker may be confirmed by visualization of coordinated, rhythmic contractions of the myocardium on the set price. Aguilera P, Durham B, Riley D: Emergency transvenous cardiac pacing placement utilizing ultrasound steerage. Problems Related to Central Venous Catheterization Inadvertent arterial puncture is a broadly known complication of the percutaneous method to the venous system. Firm compression over the puncture site will almost always end in hemostasis in 5 minutes or less. Venous thrombosis and thrombophlebitis are additionally potential problems with central venous catheterization. Thrombophlebitis, which occurs early after insertion, is an uncommon complication. Thrombosis of the innominate vein is also a uncommon problem, with pulmonary embolism being an even more unusual occasion. The choice to place a chest tube in sufferers with this complication is decided by the extent of the air leak and the scientific standing of the affected person. In addition, laceration of the subclavian vein with hemothorax,68 laceration of the thoracic duct with chylothorax, air embolism, wound infections, pneumomediastinum, hydromediastinum, hemomediastinum,sixty nine phrenic nerve harm,70 and fracture of the guidewire with embolization71,seventy two are all potential issues. Normally, the tip of the catheter ought to level anteriorly toward the apex of the center. With coronary sinus placement, the tip is displaced posteriorly and several centimeters from the sternum. Normally the tip of the catheter should level anteriorly toward the apex of the heart; nevertheless, with placement in the coronary sinus, the tip of the catheter is displaced posteriorly and several other centimeters away from the sternum. Other potential types of misplacement embody left ventricular pacing by way of an atrial or ventricular septal defect, septal puncture, extraluminal insertion, and arterial insertion. Simply pulling the catheter back and repositioning it in the right ventricle can normally deal with uncomplicated perforation. Local and systemic an infection,fifty one balloon rupture, pulmonary infarction,84 phrenic nerve pacing,eighty five and rupture of the chordae tendineae are additionally potential complications. Mechanical failures embrace displacement, fracture of the catheter, and loose leads. Displacement may find yourself in intermittent or full lack of capture or improper sensing, malignant dysrhythmias, diaphragmatic pacing, or perforation. Displacement should be suspected with modifications in amplitude, with changes of higher than ninety levels in vector, or with a change in threshold. As with displacement, catheter fractures may result in intermittent or complete loss of seize. Organic causes of pacemaker failure lead to changes in the threshold or sensing function. Electrical issues with pacing in the past have included failure of the pacemaker generator, dysrhythmias, and outdoors interference. Although ventricular tachycardia and ventricular fibrillation have been reported to end result from pacemakers, these dysrhythmias are uncommon. Therefore patients with such dysrhythmias ought to be evaluated for a non� pacemaker-induced cause. In an emergency setting, this pacing method is quicker and easier to initiate than transvenous pacing. In 1872, Duchenne de Boulogne reported profitable resuscitation of a kid by attaching one electrode to a limb whereas a second electrode was rhythmically touched to the precordium of the thorax. Zoll later launched a machine that delivered impulses lasting 2 msec through 3-cm diameter metallic paddles pressed firmly in opposition to the anterior chest wall. The original approach involving bare metal electrodes had antagonistic effects, together with local tissue burns, muscle contraction, and extreme pain.
Purchase confido 60caps
In the setting of hypoxemia duke prostate oncology purchase confido 60 caps with visa, Ti could additionally be elevated fairly exactly to increase mean airway strain and oxygenation man health urban discount confido 60caps without a prescription. Pressure-targeted modes prostate cancer 13 confido 60 caps online, that are growing in recognition, might have higher pressure distribution, improved dissemination of airway strain, and higher distribution of ventilation. Subsequent data have shown that this technique of liberation really will increase the variety of ventilator days. This might result in elevated imply airway strain, alveolar overdistention, and biotrauma. If a patient triggers the ventilator at a fee higher than the set rate, these two strategies diverge. This patient-generated breath must overcome any resistance caused by the artificial airway and ventilator circuitry. If these modes are encountered, one should focus on options with a respiratory therapist and significant care medication specialist. It is used extra generally in neonates and infants with neonatal respiratory failure. The clinician units a pressure high, a pressure low, and a time at every level (time excessive and time low). The very lengthy time at high-level pressure results in substantial recruitment of alveoli from markedly totally different regional time constants at somewhat low gasoline flow charges. This mode permits the affected person to spontaneously breathe during all phases of the cycle, thus making it comparatively extra snug and lowering the level of sedation or paralysis wanted. The patient is allowed to breathe in or out in the course of the stress excessive section and through the release section. The device shown supplies continuous positive airway stress and is run simply by attaching the masks tubing to a wall oxygen source. As the discharge phase is initiated, the move rate is recognized as adverse and is of a high rate (here, 7. Noninvasive Positive Pressure Ventilation Noninvasive air flow is defined as the provision of ventilatory assistance with out an invasive synthetic airway. Noninvasive ventilators consist of each unfavorable and positive stress ventilators. Nonetheless, adverse pressure or "iron lungs" were the mainstay of ventilatory help for sufferers with continual respiratory failure till as late because the mid-1980s. During the pressure excessive section, sufferers may exhale 50 to 200 mL or extra of gasoline as the lung quantity becomes stuffed with gasoline. The want for sedatives is reduced as a end result of patients are extra snug on this spontaneous mode than on cyclic air flow. Adjustable parameters include inspiratory optimistic airway stress, expiratory positive airway strain, and breaths per minute. On many such units, backup rates could additionally be set that ship bilevel stress, even when sufferers fail to initiate a breath. This causes preload to decrease on account of diminished venous return and likewise decreases transmural stress, which reduces afterload. In this situation, communication in regards to the expectations and objectives of care is of utmost importance. Different strategies have been utilized in scientific trials, yet these strategies have never been in contrast. This was primarily based on the concern that a depressed sensorium would predispose the affected person to aspiration. Diaz and colleagues performed an observational examine and found that success charges have been comparable between the comatose and noncomatose group. A typical nasal cannula uses a low-flow system and at larger circulate (> 6 L/min) could cause nasal dryness, epistaxis, and affected person discomfort. More research should be performed before this know-how becomes a mainstay of treatment in patients with acute respiratory failure. Vecuronium has an intermediate period of action with a half-life of 80 to 90 minutes, barely longer in the aged, however not affected by renal or hepatic failure. Vecuronium has minimal opposed cardiovascular results and is the drug of alternative for patients with cardiovascular disease or hemodynamic instability. A, High-flow flowmeter; B, oxygen blender; C, low-flow flowmeter; D, nasal cannula; E, low compliance, heated-wire circuit; F, high-flow humidifier; G, water reservoir; H, air/O2 supply. There is a average threat for antagonistic cardiovascular results related to pancuronium, such as tachycardia, hypertension, and elevated cardiac output secondary to vagal blockade. Sedation should be focused to a particular sedation scale (such as the Richmond Agitation Sedation Scale). Agents with a quick offset are preferable to enhance spontaneous awakening and for respiratory trials as quickly as the patient is a candidate for extubation. It is prudent to conclude that a paralyzed ventilated patient is awake and might hear and feel except sedated. It is important to adequately sedate these patients as a end result of their hypercapnic state is a powerful stimulus to breathe quickly. Opiates corresponding to fentanyl and sedatives similar to propofol and ketamine have gained increased roles in these sufferers. A widespread objective of blockade is to use sufficient of the agent to end in two twitches out of a "practice of 4. Valuable information can be gained from flow-time curves and pressure-time curves. The affected person has to generate a lower of only 7 cm H2O (instead of 12 cm H2O), thereby reducing the inspiratory effort required. If cardiovascular collapse happens in a ventilated asthmatic with either pulseless electrical exercise or sudden hypotension, a first step in troubleshooting is to remove the patient from the ventilator. Some clinicians also advocate fluid loading and fast and deep chest compressions while the affected person is disconnected from the ventilator to expel the excess volumes of air trapped by prior aggressive ventilation. A hyperinflated asthmatic lung severely diminishes venous return, which leads to a marked decrease in cardiac output, even pulseless electrical exercise. If a lately intubated asthmatic suffers these penalties, cease ventilating the affected person totally (arrow), compress the chest till no more air is exhaled, after which proceed ventilating as per discussion in textual content. Forty-one % of sufferers by no means acquired recommended settings throughout hospitalization. Sedation needs to be optimized, and at times completely different modes, such as pressure-targeted modes, may be attempted. In dire circumstances, these modalities could additionally be used on the premise of clinician desire and experience and session with a critical care specialist. Tension pneumothoraces could also be acknowledged by tachycardia, hypotension, elevated peak airway pressure (if mechanically ventilated, tachypnea if not), jugular venous distention, thoracic resonance by percussion on the affected facet, diminished or absent breath sounds on the affected side, and tracheal deviation away from the affected facet. Each of those catheters ought to be placed into a chest drainage assortment unit that incorporates a water seal chamber and variable suction control. Treat persistent air leaks initially with steady suction (usually suction at 20 cm H2O) to evacuate the pleural space and promote coaptation of the visceral and parietal pleurae. Reduce suction and place the chest tube on water seal only after decision of any air leak.
Purchase 60 caps confido free shipping
Intercostal space number could be decided by first palpating the sternal angle (angle of Louis) mens health 10k edinburgh discount 60 caps confido otc, which is the junction of the manubrium and body of the sternum prostate cancer medications order 60caps confido overnight delivery. This transverse bony ridge is located about 5 cm caudal from the sternal notch in adults man health advisor trusted 60caps confido. Alternatively, one can rely down from the medial aspect of the clavicle; beneath the clavicle lies the first rib, beneath which is the primary intercostal area. If the scenario demands further displacement, it is suggested that the lead be omitted, with appropriate documentation on the tracing. For occasion, the use of disposable, prewired electrodes in a fashion much like Mason-Likar positioning permits for extra speedy placement, 20% faster in comparability with standard lead placement. Adjustable Features A notation of electrocardiographic paper speed (in millimeters per second), calibration (in millimeters per millivolt), and the frequency response (in hertz) is displayed, usually within the left decrease corner of the recording. It may be manipulated for purposes of deciphering a dysrhythmia, as described later (see section on Alteration in Amplitude and Paper Speed). Calibration, or standardization, refers to the amplitude of the waveforms on the tracing. It is often set at a default value of 10 mm/mV and is graphically depicted by a plateau-shaped waveform that appears on the excessive left facet of the tracing, in entrance of the first advanced. This calibration can be modified by the operator or by the computer itself, as was the case in. Increasing the calibration to 20 mm/mV is helpful when attempting to decipher P-wave morphology. At instances calibration will be automatically adjusted by the pc primarily based on the waveform amplitudes that it perceives. In this case the calibration pulse on the left-hand aspect of the paper will have a downward stairstep look. It is important that the clinician study all electrocardiographic tracings for standardization and paper velocity parameters before rendering an interpretation. Pediatric Electrode Placement In addition to the usual 12-lead tracing, leads V4R and V3R should also be recorded; these are mirror images of their left-sided counterparts (see part on Additional Leads later in this chapter). The chest of a tiny toddler could not accommodate all the precordial electrodes; in such instances the following array is really helpful: V3R or V4R, V1, V3, and V6. On some tracings, a computer-generated interpretation, or "studying," may also be displayed on the top of the tracing. A pattern of nine of these programs was compared with the readings of eight cardiologists; the gold normal on this study was medical diagnosis made independently of the interpretations of those tracings based mostly on other goal knowledge. The efficiency of the packages was good, with right interpretations in a median of 91% of instances, but the cardiologists were significantly higher (median of 96% correct). Note the box-shaped mark to the left of the complexes (arrows); this is a graphic representation of the calibration for the tracing. The calibration on this tracing was (inexplicably and unexpectedly) changed to 20 mm/ mV by the pc, not by the operator. A was recorded minutes later with correction of calibration to the standard 10 mm/mV and was unchanged from baseline tracings. These further, or nontraditional, leads include posterior leads (V7, V8, and V9), proper ventricular leads (especially V4R), and procedural leads (transvenous pacemaker wire placement and pericardiocentesis). Place leads V7, V8, and V9 on the identical horizontal airplane as V6, with V7 at the posterior axillary line, V8 on the tip of the left scapula, and V9 close to the border of the left paraspinal muscular tissues. An further electrode, V7, may also be used and is placed on the posterior axillary line equidistant from electrode V8. Place right-sided leads V1R to V6R on the chest as a mirror image of the usual precordial leads. This alteration in lead placement is used to examine the potential of a right-sided acute myocardial infarction that may not be appreciated with normal lead placement. This affected person was discovered to have a subtotal proximal occlusive lesion of his right coronary artery at cardiac catheterization. Next, advance it until contact is made with the endocardium and the ventricle is captured. This type of monitoring will help in right positioning of the catheter within the pericardial house. In such situations, it could be necessary to place the pacing wire without the advantage of fluoroscopy. In such instances the recommendation is to advance the wire underneath electrocardiographic guidance with the patient related to the limb leads of a grounded electrocardiographic machine and the pacing wire related to the V lead (see Chapter 15). Importantly, this discount in time to management is seen in urban, suburban, and rural settings, whatever the transport time or kind of reperfusion strategy selected for the particular patient. Alteration in Amplitude and Paper Speed Most 12-lead electrocardiography machines right now allow alteration of both amplitude and paper pace from the essential 10-mm/ mV and 25-mm/sec standards, respectively. Increasing the amplitude to double the usual or 20 mm/mV, can enhance the prominence of smaller deflections such because the P wave, and might improve recognition of the atrial rhythm. This method is most advantageous when assessing patients with marked atrial or ventricular tachycardia. Increasing the paper speed exaggerates any existing irregularity (such as in atrial fibrillation) and can enhance recognition of smaller deflections, similar to P waves, in the presence of a big tachycardia. A variety of alternative lead systems requiring fewer electrodes have been described. Other various lead placements to improve detection of atrial exercise have additionally been described44�46 (Table 14. Because of the fast fee, the precise P waves are troublesome to discern, thus making determination of the rhythm difficult. In addition, the vertical sternal leads are placed over bone, which may cut back artifact brought on by muscle exercise on recordings. Limb-Precordium Leads A sequential pattern of bipolar leads on the chest, termed limb-precordium leads, has been proposed together with the unique Einthoven limb leads. Esophageal Leads the esophageal lead (E) was first described by Brown in the Thirties. Once within the esophagus, the location of the electrode is determined either by fluoroscopy or by making a collection of low to high esophageal recordings. The place of the electrode within the esophagus is adjusted by slowly pulling the electrode wire out the nares or mouth. In normal adults, leads E15�25 (the electrode is situated within the esophagus 15 to 25 cm from the nares) generally data atrial exercise; E25�35, exercise of the atrioventricular groove; and E40�50, exercise of the left ventricular posterior surface. Central Venous Catheter Intracardiac Leads For patients in whom a central venous catheter was placed for vascular entry (or for other causes similar to cardiac pacing, hemodialysis, or Swan-Ganz monitoring) that catheter, when filled with saline, can be used as a modified intracardiac electrode for recording of atrial activity. Once full of saline, a needle was then left in a facet entry port of the catheter and hooked up through an alligator clip to lead V1. A multitude of potentialities for misconnection of the limb electrodes exists; a few of the more than likely are summarized here. Reversal of the leg electrodes is largely insignificant in that the potentials at the left and right legs are primarily the same. A patient with a historical past consistent with acute coronary syndrome was delivered to the emergency division after this electrocardiogram was recorded in a clinic.
Confido 60 caps mastercard
Hematoma aspirated prostate cancer 5-alpha reductase inhibitors discount 60 caps confido, and 20-30 mL of xylocaine injected to allow painless testing of joint mobility Comminuted fracture of radial head with dislocation of distal radioulnar joint prostate health index generic 60caps confido mastercard, proximal migration of radius prostate cancer prevention trial generic confido 60 caps mastercard, and tear of interosseous membrane (EssexLopresti fracture) Ulnar n. Radial Radial recurrent branch Palmar carpal department Ulnar Anterior ulnar recurrent Posterior ulnar recurrent Common interosseous Palmar carpal department Radius Radial a. Generally, pain from overuse of the forearm extensors is called "tennis elbow," with the ache felt over the lateral epicondyle and distally into the proximal forearm. Natural lateral bowing of the radius is crucial for optimum pronation and supination. However, when the radius is fractured, the muscles attaching to the bone deform this alignment. Careful reduction of the fracture ought to try to replicate the normal anatomy to maximize pronation and supination, in addition to to maintain the integrity of the interosseous membrane. Tuberosity of radius helpful indicator of diploma of pronation or supination of radius A. Neutral Pronation Supination Normally, radius bows laterally, and interosseous house is extensive sufficient to enable rotation of radius on ulna. In fractures of radius above insertion of pronator teres muscle, proximal fragment flexed and supinated by biceps brachii and supinator muscular tissues. Malunion might diminish or reverse radial bow, which impinges on ulna, impairing capability of radius to rotate over ulna. In fractures of middle or distal radius which are distal to insertion of pronator teres muscle, supinator and pronator teres muscle tissue hold proximal fragment in neutral place. Although the carpal joints (intercarpal and midcarpal) are within the wrist, they provide for gliding actions and signiicant wrist extension and lexion. Note that the thumb (the biaxial saddle joint of the irst digit) possesses only one interphalangeal joint. Carpal Tunnel and the Extensor Compartments he carpal tunnel is formed by the arching alignment of the carpal bones and the thick lexor retinaculum (transverse carpal ligament), which covers this fascioosseous tunnel on its anterior surface. Structures passing by way of the carpal tunnel embody the next: Four lexor digitorum supericialis tendons. Synovial sheaths surround the muscle tendons throughout the carpal tunnel and permit sliding actions because the muscles contract and loosen up. Intrinsic Hand Muscles he intrinsic hand muscles originate and insert in the hand and perform ine precision actions, whereas the forearm muscular tissues and their tendons that pass into the hand are extra essential for Scaphoid (boat shaped) Lunate (moon or crescent shaped) Triquetrum (triangular) Pisiform (pea shaped) Distal Row of Carpals Trapezium (four sided) Trapezoid Capitate (round bone) Hamate (hooked bone) Metacarpals Numbered 1-5 (thumb to little finger) Two sesamoid bones Phalanges Three for every digit except thumb Chapter 7 Upper Limb 401 7 Posterior (dorsal) view Ulna Interosseous membrane Dorsal radioulnar lig. Tubercle of scaphoid Tubercle of trapezium bone Articular capsule of carpometacarpal joint of thumb Capitate Capitotriquetral lig. Although most intrinsic hand muscles are innervated by the ulnar nerve, the three thenar muscle tissue and the 2 lateral lumbrical muscle tissue (to the second and third digits) are innervated by the median nerve. Except for the thumb and lateral index inger, the remainder of the hand is provided largely by the ulnar artery. Corresponding veins drain to the dorsum of the hand and collect in the cephalic (lateral) and basilic (medial) veins. Fracture of the ulna with dislocation of the proximal radioulnar joint is termed a Monteggia fracture. The radial head usually dislocates anteriorly, but posterior, medial, or lateral dislocation also might happen. Such dislocations might put the posterior interosseous nerve (the deep branch of the radial nerve) in danger. Fractures of proximal ulna usually characterized by anterior angulation of ulna and anterior dislocation of radial head (Monteggia fracture) Anular lig. Most commonly outcomes from fall on outstretched extended hand Lateral view of Colles` fracture demonstrates attribute dinner fork deformity with dorsal and proximal displacement of distal fragment. Dorsal view shows radial deviation of hand with ulnar prominence of styloid means of ulna. Infections within the ifth digit may "seed" the frequent lexor sheath, and vice versa, through this connection. Cross part of the palm exhibits that the lengthy lexor tendons segregate out to their respective digits, creating two potential spaces (thenar and midpalmar) of the hand. Superficial palmar (arterial) arch Common flexor sheath (ulnar bursa) Superficial branch of ulnar n. Profundus and superficialis flexor tendons to 3rd digit Septum between midpalmar and thenar spaces Thenar space Flexor pollicis longus tendon in tendon sheath (radial bursa) Adductor pollicis m. On the dorsum of the digits, the extensor expansion (hood) provides for insertion of the lengthy extensor tendons and the insertion of the lumbrical and interosseous muscle tissue. Laterally, the tendons of the abductor pollicis longus and extensor pollicis brevis muscles. Long-term compression typically leads to thenar atrophy and weak spot of the thumb and index fingers, reflecting the lack of innervation to the muscular tissues distal to the median nerve harm. Distribution of branches of median nerve in hand Flexor retinaculum (roof of carpal tunnel) Flexor tendons in carpal tunnel Ulnar n. Thenar atrophy Sensory distribution of median nerve Long-term compression may end up in thenar muscle weak spot and atrophy 410 Chapter 7 Upper Limb Clinical Focus 7-17 Fracture of the Scaphoid the scaphoid bone is the most frequently fractured carpal bone and could also be injured by falling on an extended wrist. Pain and swelling in the "anatomical snuffbox" typically happens, and optimum healing depends on an adequate blood provide from the palmar carpal branch of the radial artery. Scaphoid (fractured) Trapezium Trapezoid Lunate Triquetrum Pisiform Hamulus (hook) of hamate Usually attributable to fall on outstretched hand with impression on thenar eminence Clinical findings: ache, tenderness, and swelling in anatomical snuffbox Fracture of middle third (waist) of scaphoid (most common) Because nutrient arteries only enter distal half of scaphoid, fracture typically ends in osteonecrosis of proximal fragment. Then, while compressing the radial artery with the thumb, the doctor releases the stress on the ulnar artery and asks the affected person to open the clenched fist. Normally the skin will turn pink immediately, indicating normal ulnar artery blood circulate via the anastomotic palmar arches. The take a look at is then repeated by occluding the ulnar artery to assess radial artery circulate. Clenched blanched palm Ulnar artery occluded Radial artery occluded Ulnar artery launched and patent Radial artery occluded Chapter 7 Upper Limb Extensor tendon Extensor growth (hood) 411 7 Posterior (dorsal) view Insertion of central band of extensor tendon to base of center phalanx Insertion of extensor tendon to base of distal phalanx Interosseous mm. Metacarpal bone Finger in extension: lateral view Lateral band Extensor expansion (hood) Extensor tendon Central band Lateral bands Interosseous tendon slip to lateral band Lumbrical m. Flexor digitorum profundus tendon Flexor digitorum superficialis tendon Finger in flexion: lateral view Insertion of small deep slip of extensor tendon to proximal phalanx and joint capsule Attachment of interosseous m. Flexor digitorum superficialis tendon (cut) Flexor digitorum profundus tendon (cut) Note: Black arrows indicate pull of extensor tendon; purple arrows point out pull of interosseous and lumbrical muscle tissue; dots point out axis of rotation of joints. Excessive and repetitive use of the hands in an influence grip or a twisting-wringing action could cause friction and thickening of the sheath, resulting in ache over the styloid means of the radius. This pain is mediated by the superficial radial nerve (sensory), and the pain can prolong distally into the thumb and radiate up the lateral forearm. Point of beautiful Extensor pollicis longus, tenderness over styloid strategy of Extensor pollicis brevis, radius and sheath Abductor pollicis longus tendons of involved tendons. Course of abductor pollicis longus and extensor pollicis brevis tendons via 1st compartment of extensor retinaculum, transverse incision, and relation of sensory branches of radial nerve and synovial sheaths. Superficial branch of radial nerve Extensor retinaculum Skin incision 412 supericial radial nerve, which passes subcutaneously over this area.
Purchase confido 60 caps on line
Bleeding could additionally be attributable to a ruptured aortic aneurysm androgen hormone feed loop order confido 60 caps, a ruptured myocardial infarct prostate green light laser surgery buy discount confido 60caps on line, or a penetrating injury (most frequent cause) that compromises the beating heart and reduces venous return and cardiac output prostate with grief confido 60caps generic. Coronary Arteries and Cardiac Veins he proper and left coronary arteries come up immediately superior to the proper and left cusps, respectively, of the aortic semilunar valve. During ventricular diastole, blood enters the coronary arteries to provide the myocardium of every chamber. Although variations within the coronary artery blood provide to the various chambers of the heart are widespread, normally, the proper coronary artery provides the: Right atrium. This signifies that the proper coronary artery provides rise to the inferior interventricular branch and the posterolateral artery, as shown in. In the remaining circumstances, each the best and the left coronary arteries might contribute to this branch or it may be absent and branches from each coronaries may supply this region. Inferior (posterior) interventricular (posterior descending) branch of right coronary a. Additionally, quite a few smallest cardiac veins (thebesian veins) empty venous blood into all 4 chambers of the guts, but principally into the right atrium. Chambers of the Heart he human coronary heart has four chambers, each with unique inside features associated to their perform. In each ventricles the papillary muscular tissues and their chordae tendineae present a structural mechanism that forestalls the atrioventricular valves (tricuspid and mitral) from everting (prolapsing) throughout ventricular systole. Pericardial reflection Ascending aorta Chapter 3 Thorax Right auricle (atrial appendage) Crista terminalis Septal leaflet (cusp) of proper atrioventricular (tricuspid) valve Pectinate mm. Interatrial septum Fossa ovalis Inferior vena cava Opening of coronary sinus Valve of coronary sinus Valve (eustachian) of inferior vena cava Pulmonary trunk Nonadjacent semilunar leaflet (anterior semilunar cusp) Right adjoining semilunar leaflet (cusp) Pulmonary valve Right atrium Anterosuperior leaflet (anterior cusp) Septal leaflet (cusp) Inferior leaflet (posterior cusp) Chordae tendineae Superoposterior (anterior) papillary m. Apical trabeculations Left adjacent semilunar leaflet (cusp) Conus arteriosus Septal papillary m. Chordae tendineae Coronary sinus Tricuspid valve Inferior vena cava Inferior (posterior) papillary m. Left atrium Pericardium Epicardial fats Section through left atrium and ventricle with mitral valve minimize away Left coronary leaflet (semilunar cusp) Aortic valve Right coronary leaflet (semilunar cusp) Nonadjacent leaflet (posterior semilunar cusp) Membranous septum Right pulmonary vv. This may explain why pain from visceral structures is usually mistakenly perceived as somatic ache. If indicated the doctor could prefer to use coronary angioplasty to widen the partially occluded artery, which can embody using a stent to maintain the artery open. Revascularization of the myocardium after an ischemic episode by angiogenesis, bypass surgical procedure, or percutaneous coronary intervention is important for establishing blood move to the ischemic myocardium. Recruited pericytes contribute to stabilize the three-dimensional structure of the brand new vessel. Sprouting capillary Pericytes Newly shaped blood vessels connect to each other, forming loops and increasing the capillary community. During ventricular diastole, the muscle relaxes and the tricuspid and mitral valves open usually to facilitate blood flow into the ventricles. Toward the top of ventricular diastole, the atria contract and "high of " the ventricles, just prior to ventricular systole. Cardiac Skeleton and Cardiac Valves he coronary heart has four valves that, together with the myocardium, are connected to ibrous rings of dense collagen that make up the ibrous skeleton of the center. In addition to offering attachment factors for the valves, the cardiac skeleton separates the atrial myocardium from the ventricular myocardium (which originate from the ibrous skeleton) and electrically isolates the atria from the ventricles. Second heart sound (S2): outcomes from the closing of the aortic and pulmonary valves. Necrosis usually happens approximately 20 to half-hour after coronary artery occlusion. Anterior infarct Anterolateral infarct Occlusion of proximal left anterior descending a. Infarct Infarct True posterior infarct Diaphragmatic or inferior infarct Occlusion of distal circumflex a. Sounds are best heard by auscultating the realm where turbulent blood flow radiates. Major issues embrace stenosis (narrowing) or insufficiency (compromised valve perform, typically resulting in regurgitation). Minimally vasoconstricts the coronary resistance vessels (via alpha adrenoceptors). In the posterior mediastinum, a bilateral thoracic sympathetic chain of ganglia (sympathetic trunk) passes throughout the neck of the higher thoracic ribs and, as it proceeds inferiorly, aligns itself nearer to the lateral our bodies of the lower thoracic vertebrae. Each of the eleven or 12 pairs of ganglia (number varies) is connected to the anterior ramus of the corresponding spinal nerve by a white ramus communicans (the white ramus conveys preganglionic sympathetic fibers from the spinal nerve). A gray ramus communicans then conveys postganglionic sympathetic fibers back into the spinal nerve and its anterior or posterior rami (see Chapter 1, Nervous System). Additionally, the higher thoracic sympathetic trunk conveys small thoracic cardiac branches (postganglionic sympathetic fibers from the upper thoracic ganglia, T1-T4 or T5) to the cardiac plexus, the place they mix with preganglionic parasympathetic fibers from the vagus nerve. Sympathetic ibers arise from the higher thoracic twine ranges (intermediolateral cell column of T1-T4/T5) and enter the sympathetic trunk. Cervicothoracic (stellate) ganglion Ansa subclavia Superior cervical ganglion Left vagus n. Thoracic (sympathetic) cardiac branches Cardiac plexus (deep) Thoracic (sympathetic) cardiac branches Thoracic cardiac branches of vagus n. Implantable cardiac pacemaker (dual-chamber cardiac pacing) the endocardial leads are often launched by way of the subclavian or the brachiocephalic vein (left or proper side), then positioned and tested. A pocket for the heartbeat generator is often made under the midclavicle adjacent to the venous access for the pacing leads. The incision is parallel to the inferior clavicular border, roughly 1 inch under it. The pulse generator is positioned both into the deep subcutaneous tissue just above the prepectoralis fascia or into the submuscular area of the pectoralis main. Coracoid course of Atrial and ventricular leads a hundred thirty Chapter three Thorax Clinical Focus 3-20 Cardiac Defibrillators An implantable cardioverter defibrillator is used for survivors of sudden cardiac dying, patients with sustained ventricular tachycardia (a dysrhythmia originating from a ventricular focus with a heart fee usually larger than 120 beats/min), those at high threat for growing ventricular arrhythmias (ischemic dilated cardiomyopathy), and other indications. In addition to sensing arrhythmias and offering defibrillation to stop them, the system can perform as a pacemaker for postdefibrillation bradycardia or atrioventricular dissociation. The distal coil is in the proper ventricle, and the proximal one is in the superior vena cava/right atrial place. Lesser splanchnic nerve: preganglionic fibers often come up from the T10-T11 spinal twine levels. Least splanchnic nerve: preganglionic fibers normally arise from the T12 spinal twine stage. Visceral aferents for pain or ischemia from the center are conveyed again to the higher thoracic spinal cord, normally levels T1-T4 or T5, via the sympathetic fiber pathways (see Clinical Focus 3-13).
Discount 60caps confido visa
Major problems of pacemaker placement or those caused by subsequent injuries that the emergency clinician may encounter embrace: native or systemic infections ensuing from pacemaker placement androgen hormone vs enzyme safe 60 caps confido, thrombophlebitis involving the transvenous route of the pacemaker leads prostate cancer journals 60caps confido fast delivery, a venous thromboembolic event androgen hormone yeast discount 60 caps confido amex, pneumothorax or hemothorax, pericarditis, air embolism, localized hematoma interfering with pacemaker operation or sensing, lead dislodgement, cardiac perforation, hemopericardium with possible progression to cardiac tamponade, and development of the phenomenon often identified as pacemaker syndrome. In addition to the complications related to initial pacemaker placement, malfunctions of these units may happen in the short-, intermediate-, and long-term phases of their functional life spans. Most malfunctions end result from one or a combination of three primary issues: failure of the tempo generator to present output, failure to seize, or failure to sense the intrinsic cardiac rhythm. Given that the reason for pacemaker implantation in most cases was for the treatment of an underlying bradycardia condition, preliminary scientific management of sufferers with a point of pacer output failure will usually concentrate on pharma- cologic management geared toward restoring a suitable intrinsic coronary heart price. Subsequently, a transcutaneous or transvenous pacemaker may be required to guarantee stabilization of the affected person. At this point the clinician ought to search to determine the type and mannequin of the pacemaker and should seek the assistance of an available cardiologist or electrophysiologist. Final disposition of the affected person is dependent upon the outcomes of the stabilization, diagnostic studies, and cardiology consultation, and admission is commonly required. Likewise, all class I antiarrhythmic agents (sodium channel antagonists) might have an result on pacer capture thresholds and should due to this fact be identified as potential etiologic agents in patients struggling failure to capture. If the patient is hemodynamically unstable in the setting of runaway pacemaker syndrome, it may be necessary to disconnect the pulse generator. To do that, establish the situation of the pacer leads by physical examination or a transportable chest radiograph. Dissect via the pores and skin and subcutaneous tissue after which sever the leads with a wire cutter or related software. This condition, referred to as pacemakermediated tachycardia, and alternatively as pacemaker-induced tachycardia, results most frequently from certainly one of three scientific scenarios. One caveat, however, is that sufferers with underlying coronary artery illness and countless loop syndrome may expertise coronary ischemia. A second scenario in patients with dual-chamber pacemakers happens under the circumstance in which the patient experiences an intrinsic atrial tachycardia, at which point the implanted pacemaker begins to repeatedly discharge at its most preprogrammed ventricular fee. This situation might proceed till the underlying atrial tachycardia is terminated by intervention. It appears that if this pacemaker function is switched on in such patients and an ectopic ventricular stimulus is delivered after a sudden pause in the intrinsic ventricular depolarization cycle, a ventricular tachyarrhythmia may be triggered. In the occasion of symptomatic bradycardia, placement of a magnet over the pacemaker pulse generator could additionally be indicated as a outcome of this maneuver will often place the pacemaker in an asynchronous ventricular pacing mode and thereby restore a steady and common paced ventricular rhythm whereas a consulting cardiologist or electrophysiologist is summoned. Undersensing is alleged to happen when the pacemaker fails to establish intrinsic cardiac depolarization and delivers a pacing signal. As a end result, electrocardiographic prognosis of acute ischemic changes is equally challenging in both populations. Runaway Pacemaker Syndrome this situation is seen almost solely in older pacemaker models significantly as they strategy the end of their battery life, or when the coronary heart beat generator is damaged by exposure to radiation or direct impact. The hallmark of runaway pacemaker syndrome is uncontrolled tachycardia leading to ventricular rates approaching 300 to four hundred beats/min. There is some information that a dual chamber gadget is related to a better danger of device-related issues however an analogous 1-year mortality in comparison with a single-chamber system. Suggested preliminary therapy includes the administration of amiodarone and 2-adrenergic antagonists to pharmacologically suppress the arrhythmias, and pressing cardiology consultation for attainable pacemaker interrogation, overdrive pacing, and even catheter ablation. Multiple shocks could also be a manifestation of inefficient termination of tachycardia, similar to inappropriately low-energy delivery at the first shock, elevated defibrillation thresholds, and migration or dislodgement of the defibrillation lead system, or failure of the defibrillator system. Shocks that happen each jiffy may counsel that recurring ventricular tachyarrhythmias are being terminated appropriately. Such failure could additionally be brought on by an intrinsic arrhythmia price under the programmed detection fee, normally because of concurrent pharmacologic remedy. If the affected person is hemodynamically stable, it could be advantageous for the cardiologist to interrogate the pacer earlier than initiating additional antiarrhythmic therapy. If unsuccessful or if the patient is experiencing a nonperfusing ventricular arrhythmia, different pharmacologic interventions embody procainamide or amiodarone. The affected person could have nonspecific symptoms, or have fever, localized erythema, or wound drainage. Infections happen mostly throughout the first three months of gadget implantation with the chance of severe infection and sepsis peaking at 1 month. Enterococcus is also frequent, as are gram-negative organisms, most commonly Pseudomonas. Treatment contains broad spectrum antibiotics, although localized an infection may be handled for gram-positives alone. It is believed that lowered pulse stress from continuous infusion ends in hypoperfusion of the gastrointestinal mucosa and neovascularization that, with friable vessels, is prone to bleeding. The patient could have very mild and nonspecific symptoms such as tea-colored urine to decompensated coronary heart failure. Useful laboratory tests embody coagulation research to examine for affected person compliance, and checks for hemolysis to embody a urinalysis and lactate dehydrogenase (a degree of 3 instances normal indicates hemolysis). Atrial arrhythmias ought to be treated in the identical method as the guts failure inhabitants by initially controlling the speed with -blockers. A decrease in systemic volume may end in collapse of the left ventricular wall, which may crowd the inflow cannula resulting in obstruction of blood flow (also generally known as a suction effect), and subsequent clinical deterioration. Determine the orientation of the gadget within the stomach pocket radiographically or by palpation. These sufferers are at risk for cerebral vascular events and must be treated promptly with afterload-reducing medications. The orientation of the system within the belly pocket ought to be determined, with the lead connections usually being cephalad. A ring magnet is then placed over the nook adjoining to the lead connections (usually the upper right-hand corner of the device). This practice of twiddling might lead to coiling, dislodgement, or disconnection of the pacemaker leads. At a minimum, it could end in bodily discomfort and may, actually, precipitate cardiac arrhythmias or other complications local to the location of pacemaker placement. This twisting is a direct results of the affected person "twiddling" with the gadget and will end in dislodgement or disconnection of the pacemaker leads. After preliminary stabilization of the criticism, these sufferers might require readjustment or alternative of their pacemaker units. As part of their care, pacemaker sufferers must be educated to keep away from manipulating their pacemakers. Reprogramming of operating parameters and permanent injury to the circuitry of the gadget or the electrode-tissue interface can also happen however is way much less frequent. Additional antagonistic effects which will happen embrace inhibition of bradycardia pacing, inadvertent delivery of a shock, or antitachycardia pacing. The use of hermetic shielding in steel instances, filtering, interference rejection circuits, and bipolar sensing have helped mitigate most of this interference. In addition, patients ought to be suggested to not linger in theft detection areas or airport metal detectors. Analysis of any earlier scientific event and testing of defibrillation operate are readily completed.
Order 60 caps confido otc
A much larger anterior phase turns into the hypomere (hypaxial) mass of skeletal muscle prostate cancer hormone treatment buy confido 60 caps line, which can type the muscles of the trunk wall and limb muscular tissues prostate cancer hospitals trusted 60 caps confido, all innervated by an anterior ramus of the spinal nerve mens health belly off confido 60 caps low price. Adjacent myotome segments often merge in order that an individual skeletal muscle derived from these myotomes is innervated by multiple spinal cord section. For example, the latissimus dorsi muscle is innervated by the thoracodorsal nerve, which consists of nerves from the anterior rami of spinal cord segments C6-C8. Vertebral Column Development Each vertebra irst seems as a hyaline cartilage mannequin that then ossiies, beginning in a primary ossiication heart. Ossiication facilities embody the next: Body: forms the vertebral physique; necessary for assist of body weight. Lamina Vertebral foramen Transverse course of Posterior tubercle Anterior tubercle Rib Superior articular process Body Rib ossification middle appears at eighth or 9th week. Body Pedicle Vestige of notochord Ossification heart seems at 9th or tenth week. Sacrum Superior articular process Lateral part (ala) Vestige of notochord Ossification heart seems at ninth or 10th week. Costal course of: types the ribs, or in vertebrae with out rib articulation, part of the transverse process; important for motion and muscle attachment. Neural arch: contains the pedicle and lamina, for defense of the spinal wire, and the spinous course of, for muscle attachment. Neurulation and Development of the Spinal Cord Neurulation (neural tube formation) begins concurrently with gastrulation (formation of the trilaminar embryonic disc through the third week of development). As the primitive streak recedes caudally, the midline surface ectoderm thickens to form the neural plate, which then invaginates to kind the neural groove. Embryo at 21 days (posterior view) Neural plate of forebrain Level of part Fused neural folds eighty three 2 Neural crest A. Fused neural folds 1st occipital somite 1st cervical somite 1st thoracic somite Caudal neuropore D. The trigger web site may be tender to palpation and will initiate a muscle spasm-pain-spasm cycle. Common trigger factors embrace the next muscles: Neck: levator scapulae, splenius capitis, trapezius, sternocleidomastoid Shoulder: infraspinatus, supraspinatus, rhomboid Lower back: quadratus lumborum, gluteus medius, tensor fasciae latae Thigh: biceps femoris, vastus lateralis, adductor longus Leg: gastrocnemius, soleus Deconditioning of lumbar extensors, significantly longissimus and multifidus mm. Stress Emotion Sympathetic pathways Suprasegmental facilities Sympathetic hyperactivity Gamma efferent Extrafusal fiber contraction Injury to m. Sensitivity of spindles modulated by gamma efferent system and by sympathetic innervaton of spindles. Deconditioning of extensor musculature Noxious stimuli (mechanical elements, chemical factors) Cortical processing of pain input Deconditioning of musculature due to decreased operate and disuse results in delayed repair and continued ache. Likewise, intradural myelopathies can occur from trauma, irritation, and vascular infarction (shown in this image, middle panel). Metastatic lesion Common major websites, famous on history examination Prostate Breast Myelogram exhibiting extradural block brought on by metastatic tumor Lung Melanoma X-ray movie showing (skin or destruction of mucous membrane) pedicle and vertebral physique Lymphoma by metastatic (may be carcinoma primary) Bone scan exhibiting a number of metastases Infarction Posterior columns intact (position sense infarct) Lateral corticospinal tract infarcted (motor function lost) Spinothalamic tract infarcted (pain and temperature sensation lost) because of infarction of anterolateral spinal wire because of: Thrombosis of artery of Adamkiewicz, central (sulcal) artery, anterior spinal artery, intercostal artery or to: Aortic obstruction by dissecting aneurysm or clamping throughout heart surgical procedure Sensory dissociation Loss of pain and temperature sensation Position sense retained Dissecting aortic aneurysm obstructing artery of Adamkiewicz by blocking intercostal artery Epidural abscess Pus Sources of an infection Hematogenous Dental: Urinary tract: Lung: Skin: furuncle, renal, perirenal, or pneumonia, abscess carbuncle prostatic abscess; abscess, pyelonephritis bronchiectasis Direct Throat: pharyngitis, tonsillitis, abscess Psoas abscess Dermal sinus Decubitus ulcer, direct or hematogenous Pain on percussion of backbone. Chapter 2 Back eighty five 2 Clinical Focus 2-12 Spina Bifida Spina bifida, considered one of a number of neural tube defects, is linked to low folic acid ingestion through the first trimester of being pregnant. This defect occurs most often on the L5 or S1 vertebral level and will present with neurologic findings. Spina bifida occulta Types of spina bifida cystica with protrusion of spinal contents Meningocele Meningomyelocele Clinical Focus Available Online 2-13 Myofascial Pain 2-14 Acute Spinal Syndromes Additional figures out there online (see inside front cowl for details). Besides his apparent psychological deicits, the "hunchback of Notre Dame" additionally sufered from which of the following situations You are asked to help a resident with a lumbar puncture procedure to withdraw a cerebrospinal luid sample for evaluation. A radiographic examination reveals a herniated disc between the L5 and the S1 vertebral levels. A 19-year-old man sustained an obvious cervical backbone hyperextension ("whiplash") damage after a rear-end roller-coaster crash at a local amusement park. Radiographic examination reveals a quantity of cervical vertebral body fractures and the rupture of an adjoining vertebral ligament. Which of the following vertebral ligaments was most probably ruptured throughout this hyperextension injury Anterior longitudinal ligament Cruciate ligament Interspinous ligament Ligamentum lavum Nuchal ligament 5. A 34-year-old woman presents with a spider chunk and a circumscribed space of inlammation on the back of her neck over the C4 dermatome area. A newborn female presents with a congenital neural tube defect probably attributable to a folic acid deiciency and characterised by the failure of the sclerotome to form the neural arch. Spondylolysis Multiple-choice and short-answer evaluation questions available on-line; see inside entrance cover for details. After an automobile crash, a 39-year-old man presents with a headache and midback ache. A radiographic examination reveals trauma to the thoracic spine and bleeding from the anterior and posterior inside vertebral venous plexus. A high school soccer player receives a helmetto-helmet blow to his head and neck and is introduced into the emergency division. A affected person is admitted to the emergency division with a pointy penetrating wound in the upper back region just lateral to the thoracic backbone. Based on a fast examination, the physician concludes that a quantity of of the spinal ganglia are clearly broken. Which of the following neural elements are most likely compromised by this damage A congenital defect that involves the neural crest cells would probably contain the conventional improvement of which of the next buildings Schwann cells For every of the following situations (11-20), select the muscle (A-K) most probably accountable. Erector spinae Latissimus dorsi Levator scapulae Obliquus capitis inferior Rectus capitis posterior major Rhomboid main G. A work-related damage results in a weakness in opposition to resistance in elevation of the scapula and atrophy of one of many lateral neck muscular tissues. An injury results in signiicant weakness in extension and lateral rotation alongside the complete length of the spine. After an automobile crash, a affected person presents with radiating pain around the shoulder blades and weak point in elevating the ribs on deep respiration. An harm to the again ends in a weakened capability to lengthen and medially rotate the higher limb. Sharp trauma to the again of the neck damages the suboccipital nerve, resulting in a weakened capability to prolong and rotate the pinnacle to the same aspect against resistance. Malformation of the craniocervical portion of the embryonic epaxial (epimere) muscle group that attaches to the ligamentum nuchae ends in a weakened capability to extend the neck bilaterally. Trauma to the lateral neck leads to a lesion to the dorsal scapular nerve and a weakened capability to shrug the shoulders. During spinal surgery, these small intrinsic back muscles must be retracted from the lamina and transverse processes of one or two vertebral segments. During surgery in the neck, the vertebral artery is noticed passing just deep to this muscle prior to the artery entering the foramen magnum. Hypertrophy of which of the following ligaments would most probably end result in this syndrome A 51-year-old man is admitted to the emergency department following a bicycle accident.
References
- Miller SB, Moulton M, O'Shea M, et al: Effects of IGF-I on renal function in end-stage chronic renal failure, Kidney Int 46:201-207, 1994.
- Gheiler EL, Tefilli MV, Tiguert R, et al: Predictors for maximal outcome in patients undergoing salvage surgery for radio-recurrent prostate cancer, Urology 51(5):789n795, 1998.
- Anderson JL, Adams CD, Antman EM, et al; American College of Cardiology; American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non STElevation Myocardial Infarction); American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association of Cardiovascular and Pulmonary Rehabilitation; Society for Academic Emergency Medicine: ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction. Circulation 2007;116:e148-e304.
- Illerhaus G, Fritsch K, Egerer G, et al. Sequential high dose immunochemotherapy followed by autologous peripheral blood stem cell transplantation for patients with untreated primary central nervous system lymphoma-a multicentre study by the Collaborative PCNSL Study Group Freiburg. Blood 2012, 120: abst 302.
- Luhr HG. Die Kompressions Osteosynthese Zur Behandlung Von Unterkieferfrakturen. Experimentelle Grundlagn Und Klinische Erfahrungen. Dtsch Zahnarztl Z 1972;27:29-37.
- Gassner R, Tuli T, Hachl O, et al. Craniomaxillofacial trauma in children: a review of 3,385 cases with 6,060 injuries in 10 years. J Oral Maxillofac Surg. 2004;62:399-407.
- Gnanasegaran G, Cook G, Adamson K, Fogelman I. Patterns, variants, artifacts, and pitfalls in conventional radionuclide bone imaging and SPECT/CT. Semin Nucl Med 2009;39:380-395.